COVID-19 Vaccine Myocarditis More Common and More Severe Than SARS-CoV-2 Infection Myocarditis: Landmark Study (2025)
ABSTRACT
Myocarditis, typically manifesting as myopericarditis, is among the serious cardiac consequences observed over the course of the COVID-19 pandemic. We performed a comprehensive, evidence-based literature synthesis of findings from clinical trial data reanalyses, post-marketing surveillance, large observational studies, and other diverse research sources that help shed light on the phenomenon of myocarditis post SARS-CoV-2 infection versus COVID-19 vaccine-induced myocarditis. Our conclusions refute several claims previously made by public health agencies and professional associations, namely the following: (1) the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Omicron infections have caused more cases of myocarditis than the COVID-19 mRNA immunizations; (2) mRNA vaccine-induced myocarditis is typically mild, transient, and rare, with no long-term sequelae; and (3) the risk-bene t calculus favors continued use of these products despite evidence of more iatrogenic cases. We address each of these misconceptions by applying a combination of epidemiological, clinical, and immunological perspectives. We urge governments to remove the COVID-19 mRNA products from the market due to the well-documented risk of myocardial damage, a risk that is strongest for younger males (<40 years old).
This landmark study, supported by 341 references, provides definitive evidence that COVID-19 vaccine-induced myocarditis is more common and more lethal than myocarditis caused by SARS-CoV-2 infection — decisively debunking key misconceptions promoted by public health authorities:
MAJOR MISCONCEPTIONS DEBUNKED
Misconception #1: Coronavirus Infections Cause More Myocarditis Than COVID-19 Vaccinations
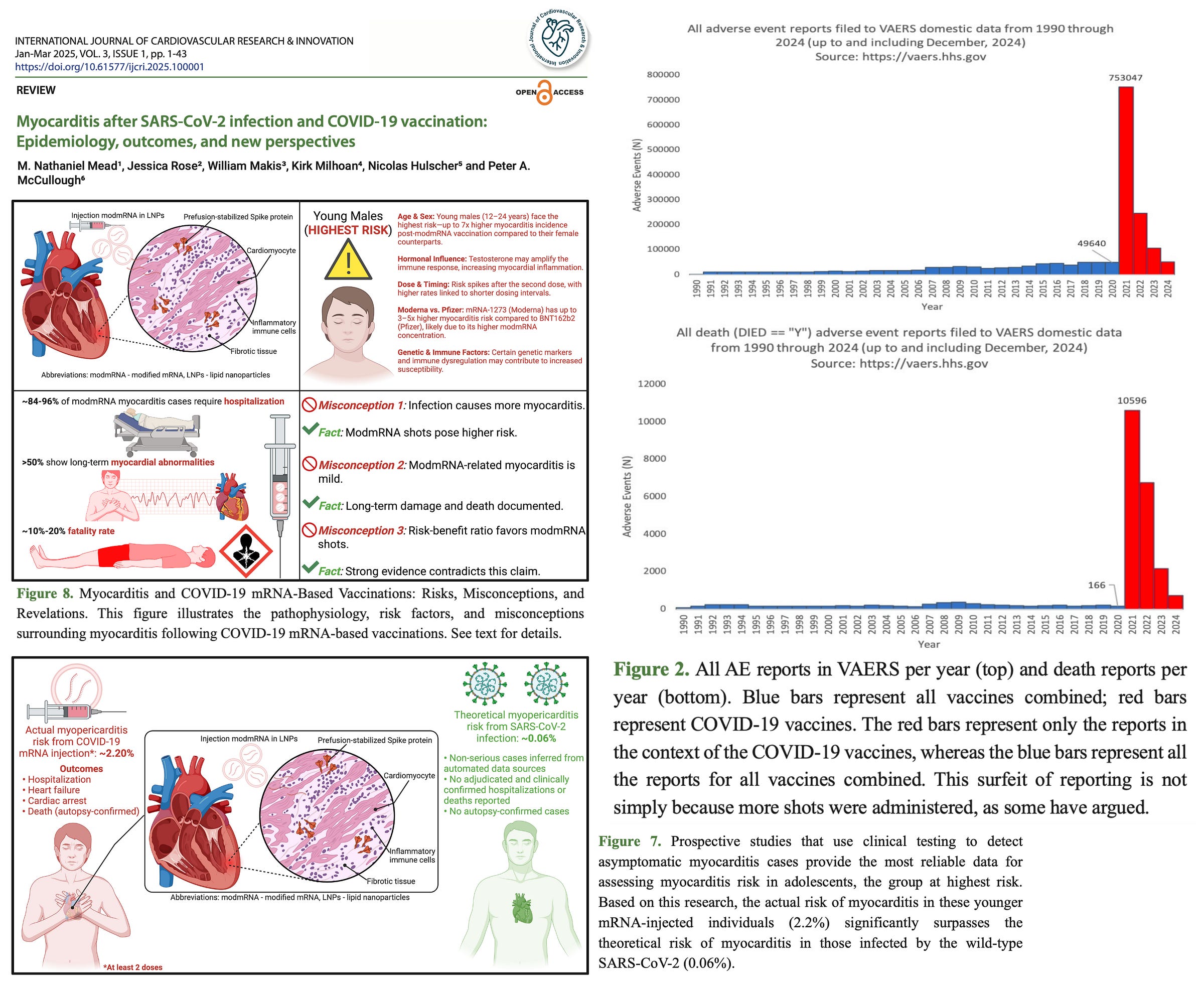
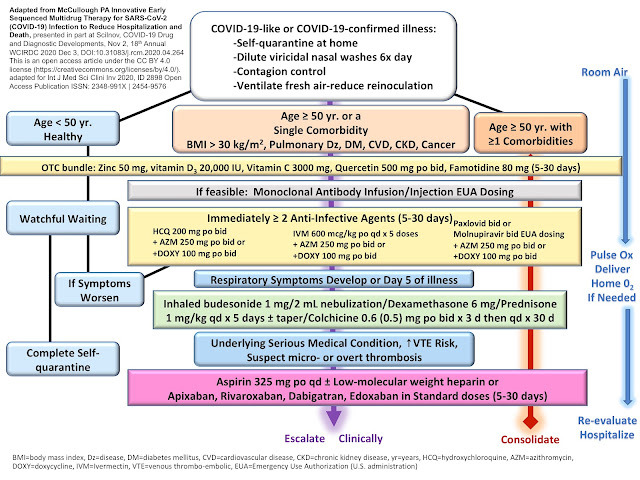
Young men (<40) were 6× more likely to develop myocarditis after the second Moderna (mRNA-1273) dose than after SARS-CoV-2 infection (97 vs. 16 cases per million).
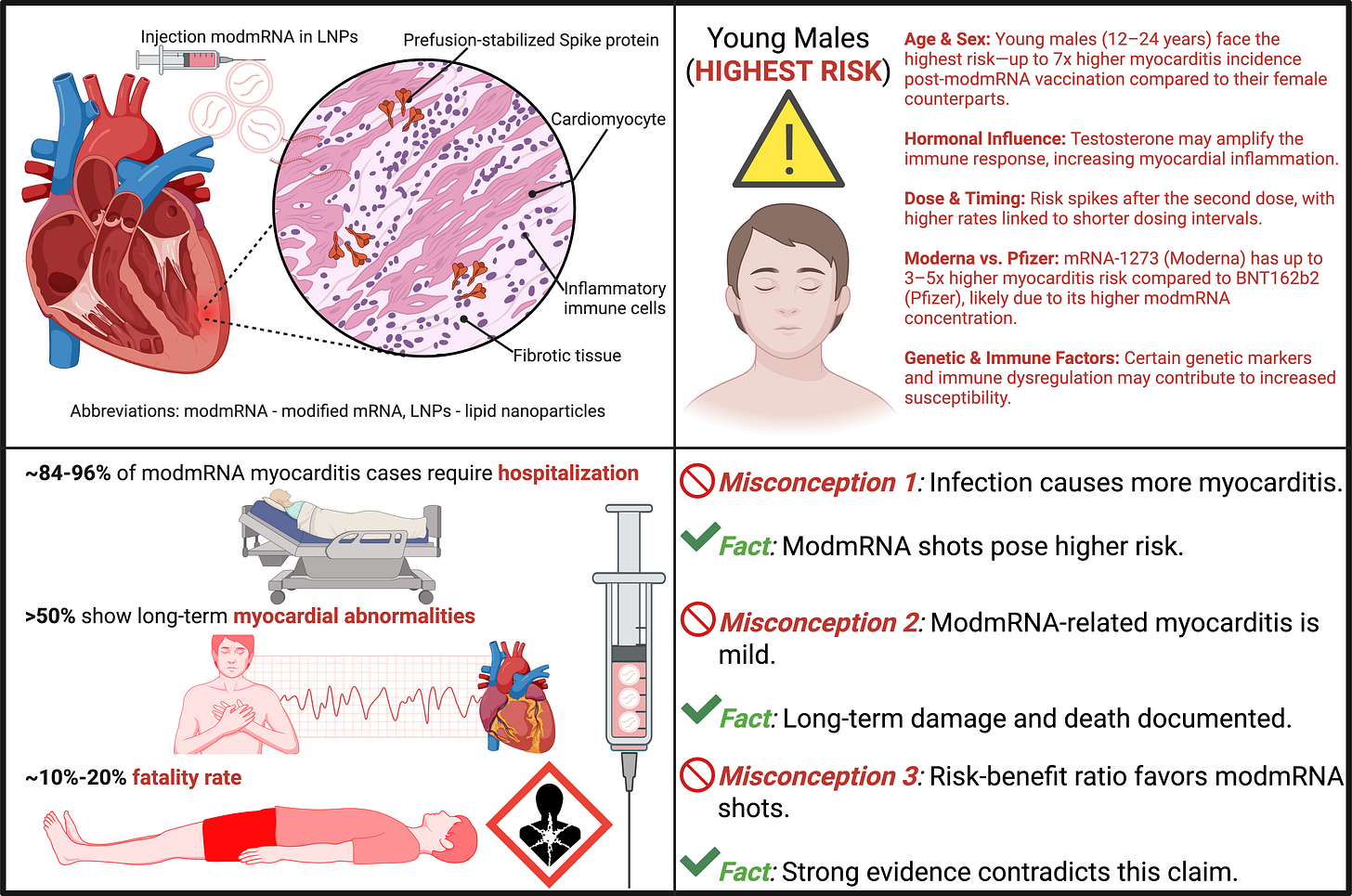
VAERS data show myocarditis reports were 223× higher following COVID-19 vaccination than the combined average for all other vaccines over the past 30 years, reflecting a 2500% increase.
From May 2021 to Nov 2024, 90% of case reports (241 out of 267) on PubMed identified mRNA vaccination—not SARS-CoV-2 infection—as the likely cause of myocarditis.
Infection-linked myocarditis estimates often relied on ICD-10 codes triggered by elevated cardiac troponins, which are non-specific markers and may result from other conditions (e.g., CAD, heart failure, or ICU-level stress).
Troponin elevations were common among ICU COVID-19 patients and frequently misclassified as myocarditis without confirmatory imaging or biopsy.
No histological confirmation (e.g., CMR or autopsy) is typically required for infection-linked myocarditis, while mRNA-associated cases are usually clinically confirmed.
The CARES Act created financial incentives (~$76,000 per case) for hospitals to classify patients as COVID-positive, which, when combined with PCR false positives and troponin tests, likely inflated infection-related myocarditis stats.
SARS-CoV-2 infection incidence is grossly undercounted due to asymptomatic or undocumented cases, leading to inflated myocarditis rates per infection (small denominator problem).
Misconception #2: COVID-19 Vaccine-Induced Myocarditis is Usually Mild and Transient
Prospective studies (Thailand, Switzerland) found 2.3%–2.8% of recipients had myocardial inflammation or injury post-mRNA dose—1 in 35 to 1 in 43, far exceeding passive surveillance estimates.
In the Swiss cohort, 2.8% showed subclinical myocardial injury after a Moderna booster; median age was 46, and half were asymptomatic, meaning these cases would escape detection in VAERS or EHR-based studies.
CDC-confirmed cases (VAERS, Dec 2020–June 2021): 96% of patients were hospitalized for myocarditis following mRNA vaccination.
Autopsy-confirmed myocarditis was responsible for 7.1% of vaccine-attributed deaths, with most deaths occurring within a week of vaccination.
More than 50% of myocarditis cases show long-term myocardial abnormalities on follow-up cardiac MRI, including late gadolinium enhancement (LGE), which is associated with risk of arrhythmia or heart failure.
Estimated fatality rate for vaccine-induced myocarditis may range between 10–20%—much higher than often reported.
Misconception #3: Risk-Benefit Analyses Favor the COVID-19 mRNA “Vaccines”
Direct cardiotoxicity of mRNA vaccines was observed in animal models (cardiomyocyte dysfunction within 48 hours). No such effect has been demonstrated with SARS-CoV-2 infection.
Vaccine-induced myocarditis often presents with acute symptoms, arrhythmias, and heart failure, requiring hospitalization. Despite hospitalization, some cases result in death. Even mild cases may cause lifelong increased risk of heart failure and sudden cardiac arrest due to residual inflammation or scarring.
Myopericarditis risk is higher in young males aged 12–24 after two doses of Moderna (mRNA-1273), requiring age-stratified analysis to avoid masking high-risk subgroups.
Fraiman et al.’s reanalysis of registrational trial data revealed 1 serious adverse event for every 800 vaccine recipients, compared to 1–2 per million for traditional vaccines—a massive safety signal not properly weighed by regulators.
The OpenSAFELY study (n=58 million) found no cases of myocarditis in SARS-CoV-2-infected children, while myocarditis occurred exclusively in vaccinated adolescents.
In the Patone et al. dataset, 16 myocarditis events occurred after vaccination in 13–17-year-olds and zero following SARS-CoV-2 infection. The study failed to analyze “day-zero” events post-vaccination and misclassified early post-dose cases as “unvaccinated,” distorting results in favor of the vaccine.
The authors highlight that infection-linked myocarditis is rare and often misdiagnosed, while vaccine-induced cases are confirmed clinically and pathologically, including via autopsy findings.
Note: The points above are not exhaustive. We encourage readers to consult the full study for the complete spectrum of evidence.
This analysis confirms that the risks of COVID-19 modified mRNA injections far outweigh any theoretical benefits, and it calls for the immediate market withdrawal of these cardiotoxic products in the interest of public health and safety.
About the Author: Nicolas Hulscher, MPH. Epidemiologist and Foundation Administrator, McCullough Foundation.






I only received one Johnson & Johnson vaccine in early 2222. I have a bone marrow cancer (not leukemia) and in the past two years received approximately 70 red cell transfusions and 60 platelet transfusions. I am recently reading about possible spike protein transference from blood donors who received one or multiple mRNA vaccines. Are there tests I can take to determine this? I’m reading about Wellness Detox, but also reading about problems bleeding. Which I already have. My platelet count is never above 7.
ReplyDelete