FLCCC I-Recover Protocol: Post Vaccine Treatment Protocol (2025)
Over the last three years, the COVID-19 pandemic has transformed almost every
aspect of our lives before we've had time to stop and question it. Although no
official definition exists for post-COVID-vaccine syndrome, a temporal
correlation between a patient receiving a COVID-19 vaccine and beginning or
worsening of clinical manifestations is sufficient to diagnose as a COVID-19
vaccine-induced injury, when the symptoms are unexplained by other concurrent
causes.
Dr. Paul Marik and Dr. Pierre Kory are pleased to introduce the I-RECOVER:
Post-Vaccine Treatment protocol, designed to help people who have experienced
adverse symptoms after a COVID vaccine.

Note that there are significant overlaps between the symptoms and features
of long COVID/long-hauler syndrome
and post-vaccine syndrome. However, a number of clinical features appear
to be characteristic of post-vaccine syndrome; most notably, severe
neurological symptoms appear to be more common following vaccination. To
complicate matters further, patients with long COVID are often also
vaccinated, making the issue of definition more difficult.
Since there are no published reports detailing the management of
vaccine-injured patients, the FLCCC treatment approach is based on the
postulated pathogenetic mechanism, clinical observation, and patient
anecdotes. Treatment must be individualised according to each patient’s
presenting symptoms and disease syndromes. It is likely that not all
patients will respond equally to the same intervention; a particular
intervention may be life-saving for one patient and totally ineffective
for another. Early treatment is essential; it is likely that the response
to treatment will be attenuated when treatment is delayed.
Updates:
- Niclosamide vs Methylene Blue for Spike Protein Disease (2025)
- Effects of nicotinamide riboside on NAD+ levels, cognition, and symptom recovery in long-COVID: a randomized controlled trial (Lancet Nov 2025)
Two Strategies to Eliminate Spike Protein
Marik and Kory believe there may be ways to boost the immune system to allow it to degrade and eventually remove the spike from your cells. One of the strategies they recommend for this is TRE (time restricted easting), which stimulates autophagy, a natural cleaning process that eliminates damaged, misfolded and toxic proteins.Ivermectin also binds to the spike protein, thereby facilitating its removal. The spike protein is toxic regardless of whether it comes from the natural infection or the injection. Early and aggressive treatment will lower your spike protein load, thereby reducing your risk of long-COVID.
Kory stresses that, at present, they still do not know the exact correct dose for ivermectin. When prescribed for long-COVID and vaccine injury, he monitors the patient and adjusts the dosage based on individual response. That said, he typically starts patients out at a mid-range dose of 0.3 milligrams per kilogram of bodyweight, daily.
Now, he's noticed that when it comes to ivermectin, there are responders and non-responders. It works exceptionally well for some, while benefits are negligible in others. That said, a majority of patients do tend to experience a benefit. The length of treatment is also highly variable.
As for safety, it's been used for over 50 years and has a remarkably robust safety profile. We now also have a large-scale Brazilian study in which patients received ivermectin for four days every month for six months. Curiously, not only was COVID incidence dramatically reduced, but kidney and liver function actually improved with this treatment. Marik also dismisses claims that ivermectin can be harmful to your liver, saying it's actually used to treat fatty liver disease.
So, overall, "we have not seen a safety signal ... with long-term use," Kory says. "Some of that is published data, and some of it is just our experience with treating patients." Marik adds, "It's one of the safest medications ... even when taken in high doses appropriately."
The FLCCC (Front Line COVID-19 Critical Care Alliance) was formed by
leading critical care specialists in March 2020, at the beginning of the
Coronavirus pandemic, dedicated to developing highly effective treatment
protocols to prevent the transmission of COVID-19 and to improve the
outcomes for patients ill with the disease.
Though there are many long haulers treatment protocols out there, we
consider and recommend the I-Recover protocol as one of the best.
Given the lack of clinical trials of long-haul COVID-19 syndrome,
these recommendations are based on the abnormal changes within the
body associated with the COVID-19 disease and post viral illnesses
along with the collective experience of FLCCC members.
This protocol has also been used to treat post-vaccine inflammatory
syndromes with similar success. As with all FLCCC Alliance protocols,
the components, doses, and durations will evolve as more clinical data
accumulates.
Note that there are two post-vaccine protocols, one to
treat post vaccine injury (I-Recover Post Vaccine) and the
other to prevent post vaccine injury (I-Prevent Post Vaccine).
Patients with post-vaccine syndrome should do whatever they can to prevent themselves from getting COVID-19. This may include a preventative protocol (see I-PREVENT) or early treatment in the event you do contract the virus or suspect infection (see I-CARE). COVID-19 will likely exacerbate the symptoms of vaccine injury.
Once a patient has shown improvement, the various interventions should be reduced or stopped one at a time. A less intensive maintenance approach is then suggested.
The core problem in post-vaccine syndrome is long-lasting “immune dysregulation.” The most important treatment goal is to help the body restore a healthy immune system — in other words, to let the body heal itself. Our recommended treatment strategy involves two major approaches:

About Ivermectin
"She took Ivermectin...her inflammation, iron, pericarditis all back to normal, the blood clots gone, her appetite has returned and she can now walk for 50 mins around the block daily :) Thank you for your advice. I am extremely grateful and may God bless you and your family"
According to Dr William Makis:
"Why 0.5mg/kg/day? It's the upper range of established dosing for anti-viral and anti-parasitic indications. With minimal risk of side effects."



Treatment must be individualized according to each patient’s
presenting symptoms and disease syndromes. It is likely that not
all patients will respond equally to the same intervention; a
particular intervention may be life-saving for one patient and
totally ineffective for another. Early treatment is essential;
it is likely that the response to treatment will be attenuated
when treatment is delayed.
Patients with post-vaccine syndrome should do whatever they can to prevent themselves from getting COVID-19. This may include a preventative protocol (see I-PREVENT) or early treatment in the event you do contract the virus or suspect infection (see I-CARE). COVID-19 will likely exacerbate the symptoms of vaccine injury.
Once a patient has shown improvement, the various interventions should be reduced or stopped one at a time. A less intensive maintenance approach is then suggested.
The core problem in post-vaccine syndrome is long-lasting “immune dysregulation.” The most important treatment goal is to help the body restore a healthy immune system — in other words, to let the body heal itself. Our recommended treatment strategy involves two major approaches:
- Promote autophagy to help rid the cells of the spike protein
- Use interventions that limit the toxicity/pathogenicity of the spike protein
Note: The I-Recover protocol has been updated and below is their latest version, based on the FLCCC document called “An Approach to Managing Post-Vaccine Syndrome” (March 2024).
First Line Therapies
(Not symptom specific; listed in order of importance)- Intermittent daily fasting or periodic daily fasts. (Read more)
- Ivermectin : 0.2 - 0.3 mg/kg daily. (Stone 2022) (Find Provider)
- Moderating physical activity.
- Nattokinase (McCullough 2023, Jose Crespo-Barrios 2025): 100-200 mg (2000- 4000 Fibrinolytic Units) twice daily.
- L-Arginine (1.5 -2g twice daily) and Vitamin C (1000 mg orally two to three times daily)*
- Low-dose naltrexone: 1- 4.5 mg daily.
- Treatment of Mast Cell Activation.
- Sunlight and Photobiomodulation (Red Light Therapy)
- Melatonin: 2-6 mg slow release/extended release prior to bedtime
- Bromelain + NAC (Amazon)
- Nigella sativa (Black Seed Oil)
- Resveratrol or a combination flavonoid
- Probiotics/Prebiotics (Lau 2023)
-
Vagus Nerve Stimulation and nicotinic agonists
- Metformin (COVID-OUT 2023)
*Liposomal Vitamin C (Amazon) or whole food vitamin C (PaleoValley Essential C Complex): 1000 mg orally two to three times a day.

Second-Line Therapies
(Listed in order of importance)
- Vitamin D3 (4000-5000 units/day) and Vitamin K2 (100 mcg/day).
- N-acetyl cysteine (NAC): 600-1500 mg/day
- Cardio Miracle™ and L-arginine/L-citrulline supplements
- Omega-3 fatty acids: FLCCC suggest a combination of EPA/DHA with an initial dose of 1 g/day (combined EPA and DHA) and increasing up to 4 g/day (of the active omega-3 fatty acids).
- Triple anticoagulation
- Magnesium
- Sildenafil (with or without L-arginine and L-citrulline)
- Spermidine
- Non-invasive brain stimulation
- Intravenous Vitamin C: 25 g weekly, together with oral Vitamin C 1000 mg (1 gram) 2-3 times per day. (Find Provider)
- Behavioral modification, relaxation therapy, mindfulness therapy, and psychological support
Third Line Therapies
- Hyperbaric oxygen therapy (HBOT)
- Low Magnitude Mechanical Stimulation
- “Mitochondrial energy optimizer” with pyrroloquinoline quinone, glycophospholipids, CoQ10, NADH, and other nutrients (e.g., Life Extension Energy Optimizer, Restorative Solutions Mitochondrial Nutrition PQQ, Researched Nutritionals ATP 360® and ATP Fuel® and PureEncapsulations Mitochondria-ATP)
- Low-dose corticosteroid
Warning (anaesthesia and surgery):
Patients should notify their anesthesia team if using the
following medications and/or nutraceuticals, as they can
increase the risk of Serotonin syndrome (SS) with opioid
administration:
.png)
- Methylene blue
- Curcumin
- Nigella Sativa
- Selective Serotonin Reuptake Inhibitors (SSRIs)
Note: There are also some important cautions and
contraindications that should be carefully reviewed within
the more comprehensive and detailed document called “An Approach to Managing Post-Vaccine Syndrome” (March 2024) and which should be discussed with a
qualified provider as well.
.png)
About Ivermectin
Ivermectin is a well-known, FDA-approved drug that has been used successfully around the world for more than four decades. One of the safest drugs known, it is on the WHO’s list of essential medicines, has been given over 3.7 billion times, and won the Nobel Prize for its global and historic impacts in eradicating endemic parasitic infections in many parts of the world.
Review the totality of supporting evidence for ivermectin: https://c19ivm.org.
Review the totality of supporting evidence for ivermectin: https://c19ivm.org.
It is likely that ivermectin and intermittent fasting act
synergistically to rid the body of the spike protein.
It appears that vaccine-injured patients can be grouped into two categories: i) ivermectin responders and ii) ivermectin non-responders. This distinction is important, as the latter are more difficult to treat and require more aggressive therapy.
For ivermectin responders, prolonged and chronic daily treatment is often necessary to support their recovery. In many, if the daily ivermectin is discontinued worsening symptoms often recur within days.
It appears that vaccine-injured patients can be grouped into two categories: i) ivermectin responders and ii) ivermectin non-responders. This distinction is important, as the latter are more difficult to treat and require more aggressive therapy.
For ivermectin responders, prolonged and chronic daily treatment is often necessary to support their recovery. In many, if the daily ivermectin is discontinued worsening symptoms often recur within days.
Ivermectin is best taken with or just following a meal, for
greater absorption.
High dose ivermectin
Dr William Makis shared a case of vaccine injury that was successfully treated with high dose ivermectin:
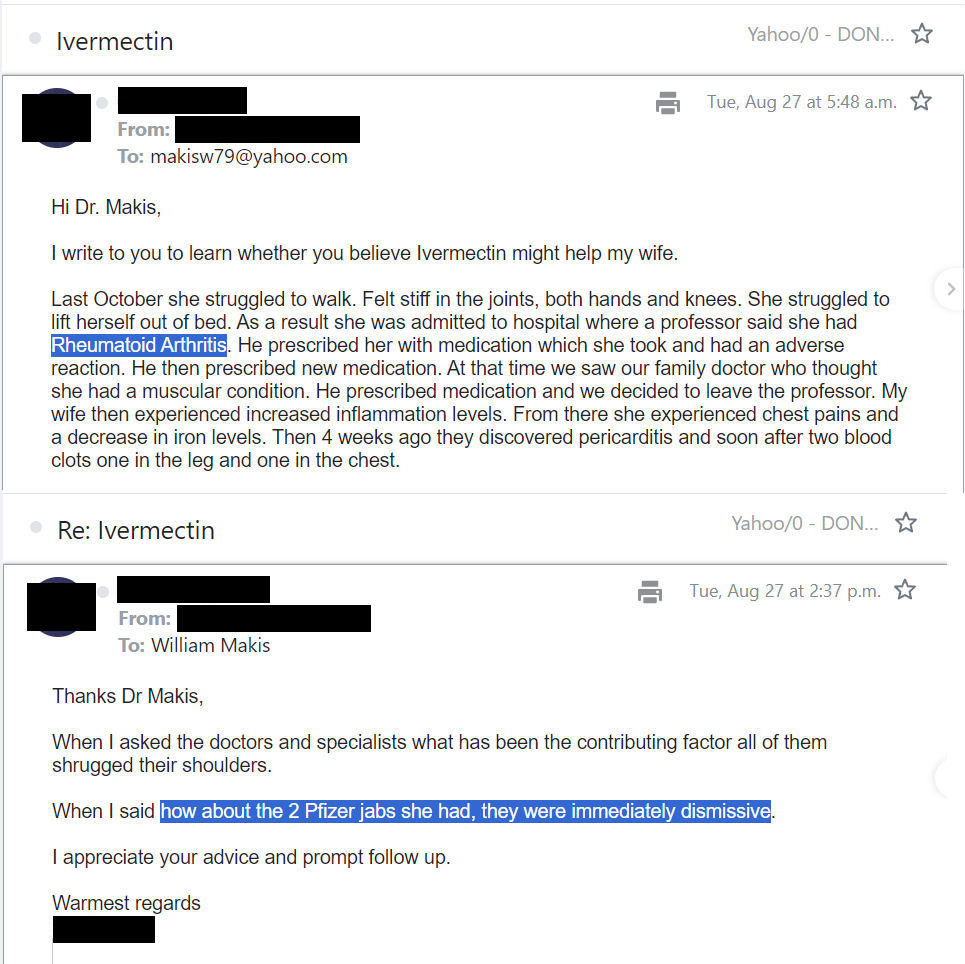
IVERMECTIN Testimonial - Pfizer COVID-19 mRNA Vaccine Injuries - Young Australian woman recovers from multiple mRNA Vaccine injuries (polyarthritis, pericarditis, blood clots, and more) in 2 months!
"In August 2024, an Australian couple reached out to me. The wife had two Pfizer COVID-19 mRNA Vaccines and began suffering inexplicable side effects in late 2023."
"She struggled to walk. Felt stiff in the joints, both hands and knees. She struggled to lift herself out of bed. She was admitted to hospital where a professor said she had Rheumatoid Arthritis...family doctor thought she had a muscular condition she experienced chest pains...pericarditis and soon after two blood clots one in the leg and one in the chest"
"Australian doctors were baffled (of course). "When I asked the doctors and specialists what has been the contributing factor, all of them shrugged their shoulders. When I said how about the 2 Pfizer jabs she had, they were immediately dismissive"
I suggested Ivermectin 0.5mg/kg/day for several weeks.
A few days ago, I heard back from them


How to Order Your Own Spike Antibody Test
You can now order a Spike protein antibody test from Labcorp Labs On Demand and get the results within a few days.
Here is a quick guide of interpretation of your results:
- <1000 U/ml very low level past exposure, negligible risks
- 1000-5000 U/ml symptoms or problem could be related to Spike protein
- >5000 U/ml Spike protein likely circulating in your bloodstream
- 10,000-25,000 U/ml very high risk for cardiac damage, blood clots, neurologic problems, autoimmunity, and potentially cancer

Other Options
You can also order a Spike antibody (Covid-19 antibody) test from healthlabs.com to assess your risk and establish a baseline before and after starting any anti-spike protein protocol.
Another option is Attomarker's COVID Antibody Spectrum Test. Although the test is now available for sample collection in the US, the actual testing is still performed in the UK (United Kingdom). Please note that the test report takes about 2 to 3 weeks to arrive (X.com). The COVID Antibody Spectrum Test measures antibody levels & quality to Spike variants. Mapped with variant prevalence & your medical history, it offers insights into your immune profile, and has helped people with long COVID explore treatment pathways.
Related: The Protective Role of Healthy Lifestyles Against SARS-CoV-2 and Other Viral Infections: A Systematic Review of 119 Studies.
Disease-Specific Therapeutic Adjuncts
Generalized Neurologic Symptoms/Injuries/“Brain Fog”/Fatigue
- LDN (low dose naltrexone) appears to play a pivotal role in treatment of many neurological symptoms
- Fluvoxamine; Start on a low dose of 12.5 mg/day and increase slowly as tolerated. Some patients report a significant improvement with fluvoxamine while other patients appear to tolerate this drug poorly. Fluoxetine 20 mg/day is an alternative, as are tricyclic antidepressants.
- Nigella Sativa; 200-500 mg twice daily.
- Valproic acid and pentoxifylline may be of value in these patients.
- These symptoms may be mediated by Mast Cell Activation Syndrome (MCAS); see specific treatment below.
- Luteolin: Long-COVID syndrome-associated brain fog and chemofog: Luteolin to the rescue [R].
Note: Ivermectin is not thought to readily cross the blood-brain
barrier in humans as it is excluded by a P-glycoprotein drug pump
(mdr-1). (PubMed)
Patients with new onset allergic diathesis and those with features of Mast Cell Activation Syndrome (MCAS)
- The novel flavonoid lutein is reported to be a potent mast cell inhibitor. [R] Lutein 20- 100 mg/day is suggested.
- Turmeric (curcumin); 500 mg/day. Curcumin has been reported to block H1 and H2 receptors and to limit mast cell degranulation. [R]
- H1 receptor blockers. Loratadine 10 mg/day, Cetirizine 5-10 mg/day, Fexofenadine 180 mg/day.
- H2 receptor blockers. Famotidine 20 mg twice daily as tolerated. [R]
- Vitamin C; 1000 mg twice daily. Vitamin C is strongly recommended for allergic conditions and MCAS. Vitamin C modulates immune cell function and is a potent histamine inhibitor.
- Low histamine diet.
- Montelukast 10 mg/day. Caution as may cause depression in some patients. The efficacy of montelukast as a “mast cell stabilizer’ has been questioned. [R]
Patients with an elevated DIC and those with evidence of thrombosis
- These patients should be treated with a NOAC (novel anti-coagulants) or coumadin for at least three months and then reevaluated for ongoing anticoagulation.
- Patients should continue Aspirin 81 mg/day unless at high risk of bleeding.
- Lumbrokinase activates plasmin and degrades fibrin. e.g., Lumbroxym (US Enzymes). [R] Lumbrokinase appears to be well absorbed from the GI tract. [R]
- Turmeric (Curcumin) 500 mg BID. Curcumin has anticoagulant, antiplatelet and fibrinolytic properties. [R]
- Triple anticoagulation should be considered in select patients. [R] Treat no longer than one month. Triple anticoagulation increases the risk of serious bleeding; patients should be counselled regarding this complication.
- In those patients with marked microvascular disease/thrombosis, the combination of pentoxifylline and sildenafil should be given a therapeutic trial. [R]
Treatment protocol for Vaccine induced myocarditis/pericarditis
- ACE inhibitor/ARB, together with carvedilol as tolerated to prevent/limit progressive decline in cardiac function.
- Colchicine in patients with pericarditis – 0.6 mg/day orally; increase to 0.6 mg twice daily if required. Reduce dose if patients develop diarrhea. Monitor white blood cell count. Decrease dose with renal impairment.
- Coenzyme Q (CoQ) 200-400mg/day. (R, R, R)
- Omega-3 fatty acids – EPA/DHA 1-4 g/day (R). Increase dose slowly as tolerated.
- Referral to a cardiologist or ER in case of persistent chest pain or other signs and symptoms of cardiac events are observed.
Herpes virus reactivation syndrome
- L-Lysine; 1000 mg twice daily [R]
- Valtrex; 500-1000 mg twice daily for 7-10 days (acyclovir is an alternative). [R]
- Spironolactone 50-100 mg daily [R]. Spironolactone has antiviral properties against Epstein Barr Virus by inhibiting viral capsid antigen synthesis and capsid formation. Spironolactone likely has antiviral effects against other Herpes viruses.
- Zinc 40 mg daily [R]
- Quercetin 500 mg twice daily (as a Zinc ionophore) [R]
Note: Herpes simplex virus, that causes cold sores, requires
arginine (amino acid) to replicate and thrive in your body.
Depriving the virus of arginine can certainly reduce the
duration and severity of an outbreak. Foods that contain
arginine include flaxseeds, sunflower seeds, sesame seeds,
chocolate, spinach, whole grains, almonds, peanuts, hazelnuts
and walnuts. Avoid these foods completely when you feel the
first few symptoms of a cold sore. [R]
A cold sore outbreak cannot be stopped once you have it. What you can do is eat food that helps in preventing the outbreaks. Lysine (amino acid) blocks arginine, and stops the virus from replicating. Lysine-rich foods like vegetables, legumes, milk, cheese and fish are helpful in strengthening your immune system and preventing cold sore.
A cold sore outbreak cannot be stopped once you have it. What you can do is eat food that helps in preventing the outbreaks. Lysine (amino acid) blocks arginine, and stops the virus from replicating. Lysine-rich foods like vegetables, legumes, milk, cheese and fish are helpful in strengthening your immune system and preventing cold sore.
Tinnitus
- This a frequent and disabling complication reported in post-vaccine syndrome. (R)
- Tinnitus refers to the sensation of sound in the absence of a corresponding external acoustic stimulus and can, therefore, be classified as a phantom phenomenon. Tinnitus sensations are usually of an unformed acoustic nature such as buzzing, hissing, or ringing. Tinnitus can be localized unilaterally or bilaterally, but it can also be described to emerge within the head. [R]
- Ideally, patients should be evaluated by an ENT specialist or audiologist to exclude underlying disorders.
Vision Impairment and Migraines
- These are lesser known adverse events that are appearing in the research literature as well as in doctors’ clinics. (R)
- Patients should be evaluated by an Eye specialist or neurologist to exclude underlying disorders.
Bell’s Palsy / Facial Paresthesia
- Low dose naltrexone (LDN). Begin with 1 mg/day and increase to 4.5 mg/day as required. May take 2-3 months for full effect.
- Low dose corticosteroid: 10-15 mg/day prednisone for 3 weeks. Taper to 10 mg/day and then 5 mg/day as tolerated.
- Reduced workload, stress, and light exercises for a couple of months.
IVIG treatment (Intravenous immunoglobulin treatment)
- Generally, treatment with IVIG is not recommended.
Immunosuppressive Therapies
- As a rule, immunosuppressive therapy should be avoided, as these drugs may exacerbate the immune dysfunction in vaccine-injured patients and prevent restoration of immune homeostasis.
- A trial of immunosuppressive therapy may be indicated in patients with an established autoimmune syndrome who have failed other therapeutic interventions.
IMA/FLCCC protocols
This protocol is solely for educational purposes regarding potentially beneficial therapies for COVID-19. Never disregard professional medical advice because of something you have read on our website and releases. This protocol is not intended to be a substitute for professional medical advice, diagnosis, or treatment with regard to any patient. Treatment for an individual patient should rely on the judgement of a physician or other qualified health provider. Always seek their advice with any questions you may have regarding your health or medical condition. Please note FLCCC's full disclaimer at: www.flccc.net/disclaimer.
Read more articles related to spike protein > Spike Protein series
- Fact Check: Unpacking the Spike Protein Debate (2025)
- Evidence linking vaccines to autism (110 studies) (X.com 2025)
- American woman fired for refusing COVID-19 vaccine wins $13 million lawsuit. (2024)
The Wellness Company's Base Spike Detox Trio
.png "The Wellness Company's Base Spike Detox Trio")
The first ever spike detox protocol appeared in the US Medical Literature and now it is available to you!
This base spike protein detox protocol consists of these three powerful ingredients: Spike Support's Nattokinase, Bromelain, and Tumeric Extract.
Vaccinated or not, prioritizing your well-being has never been more crucial.
Buy this ultimate detox bundle today, researched by Dr. Peter McCullough.
Recommended to maintain daily health for anyone exposed to COVID, vaccines, or shedding – and may help your body repair itself and remain at optimal health.
Where to buy Base Spike Detox Trio Formula: Available on The Wellness Company's website. Here is the link: Base Spike Detox Trio
Note: To get 10% OFF, please use this coupon code: ONEDAYMD







.png)
Can you tell me if an unvaccined person has intimacy with an vaccined person is there risk or harm transfered to the unvaccined person from the vaccined? Thank you
ReplyDeleteAn unvaccinated person can be affected through vaccine shedding of a vaccinated person. No intimacy is required. There are things you can do, as noted on this page. The Spike Support formula would be very helpful to the unvaxxed (as you can read in the comments section).
DeleteCan you tell me or direct me to information how to remove the harm from the vaccine from the body. Thank you
ReplyDeleteIs there a blood test that determines how much vax damage I may have? Or are these protocols guess work?
ReplyDeleteHi, Two days after my second Pfizer vaccine, my body has been on the decline. For three years I have spend thousands of dollars and been to many different doctors. None will discuss the vaccine causing my health decline. I have recently been diagnosed with the stage before Multiple Myeloma. Extremely high IGA, spike protein, low WBC, etc. I have no oil in my body at all. I test negative for Sjogren’s. My mouth is so dry my gums have started to recede, eyes are so dry I no longer can walk through the grocery aisles. Eye drops of any kind may help for .05-1 second and then extremely uncomfortable again as I need oil. My back is in constant pain and the fatigue has prevented most of my life quality. I bruise and bleed easily and my circulation seems to be poor, especially when my feet are concerned. I was diagnosed with psoriasis and my fingers and toes hurt to be used for any length of time. Endoscopy shows ulcers and lesions in my digestive track. I literally feel like I am dying. I currently have an oncologist and rheumatologist but neither have shown desire to help. I was prescribed Hydroxychloroguine 200mg twice daily. I am going to start taking the three OTC medications suggested here and I pray I can recover, even if just enough to regain some quality of life. I have my journey documented from the beginning to current. I would love to help in any way with your study and or research. I am open to paying for my own transportation and lodging if you would be willing to speak with me one on one. My email is lorimbarbery at gmail dot com if you would like to contact me. Thank you so very much for the information you have shared.
ReplyDeleteI hope you find the healing you are seeking. Dr. McCullough’s email is listed elsewhere on this site:
DeletePeterAMcCullough@gmail.com
I would not continue treatment with any medical doctor, especially the oncologist and I don’t much about rheumatologists but they are all the same. You need a functional medicine doctor to heal your body! Medical doctors are controlled by big pharma and they will never acknowledge a vaccine injury unless it is so blatantly obvious (medical emergency minutes after shot.)
DeleteFollow the detox protocols. Get vitamin C IVs with glutathione and EDTA.
DeleteTake ivermectin.
Use nicotine patches daily to release the venomous peptides from the acetacholine receptors.
Take all recommended supplements.
God bless you.
I will keep you in my daily prayers.
Have you tried the ivermectin! I would do it for 7 days straight then go to the 4 days a month for at least 4 months then see how you feel! Good luck I hope you find the help you need!
DeleteI'm a bedside nurse. I did not took the jab and was blessed to keep my job. However, I work among many people that is fully vaccinated. Most of my patients are too. Is there any precautions I can take from the vaccine shedding? Also, how.much ivermentin as a preventive measure should I take weekly
ReplyDeleteThank you so much for your excellent job and commitment to health after the pandemic chaos.