Health Implications of Poor COVID-19 mRNA Testing: Miscarriage, Vision Loss, Immunotoxicity
Summary of Key Facts:
- The COVID-19 mRNA vaccines were authorized for human use without going through complete animal testing on the active ingredients.
- The animal testing data, which we review in detail, shows that the mRNA and LNP shell are present in tissues at high concentrations for about 72 hours, consistent with the timing of systemic reactions to vaccination within the first two to three days.
- The lipids used to create the LNP shell likely stay in the body for four to five months due to their long half-life. (pdf)
- Details on animal testing also show elevated adverse event rates, including joint inflammation and early pregnancy loss.
- The regulatory authorities knew about these adverse events found in animals by January 2021. Nevertheless, the products were permitted to go forward in humans, assuming the benefits would outweigh the risks.
- Post-licensure studies on rare adverse events have found evidence of post-vaccination myocarditis, neurological issues, thrombocytopenia (low platelet counts), and clotting, and a new study shows a strong, twofold increased risk of vision loss.
False Reassurances From CDC
As discussed in Part 1, the U.S. Food and Drug Administration (FDA) did not require Pfizer and Moderna to do biodistribution testing on the active mRNA encoding spike protein used in the vaccines. The FDA’s relaxed biodistribution and pharmacokinetic testing essentially approved a “bioengineered egg” based on an examination of the shell only; in other words, the contents were not tested.
Reports provided by Pfizer to the FDA (pdf), Australian, and Japanese (pdf) health authorities, as well as the European Medicines Agency (EMA) (pdf) in January 2021 include identical animal data showing how the new LNP shell travels throughout the body. The reports also show how a substitute (“fake”) mRNA (encoding for luciferase) was used to visualize where the mRNA travels.
Although the compound luciferase has a sinister name, it is a harmless enzyme found in fireflies and elsewhere in nature, and it is bioluminescent—meaning, it glows in the dark. Thus, luciferase is useful for visualizing biological compounds in animal tissues.
These reports show widespread dispersal of the LNP shell. The CDC gave false reassurances about the duration of biological activity and distribution based on scant data on animals and no human data on biodistribution. People relied on these statements as truth. Thus the agency disseminated vague and misleading reassurances when data was available at the time, which contradicted these claims.
Although the CDC’s original webpage, now only available through web archives, contained a message stating that mRNA is broken down within days and that the spike protein does not persist in the body beyond a few weeks—we simply did not have this data, presumably leading them to remove the highlighted duration reference.
To understand the health implications of the new mRNA vaccine technology, we must first examine where luciferase, the spike protein, and the LNPs travel in the body and how long they persist.
What Happens to the ‘Glow-in-the-Dark’ Luciferase?
The European Medicines Agency (EMA) is the European Union’s FDA equivalent. The EMA report (pdf) gives us more detail about animal studies showing where the luciferase and LNP shell travel, as well as the concentrations of these compounds in tissues immediately after vaccination.
Pfizer conducted a study using two approaches—bioluminescence and radioactivity–to tag the mRNA for luciferase and the LNP shell for radioactivity.
The luciferase mRNA signals peaked at the injection site within six hours, at 10,000 times that of the control animals. Luciferase activity was also found in lymph nodes and the liver. The signal then decreased slowly over 72 hours. (page 46) Levels continued to decline and by day nine, the luciferase level in the experimental animals was seven times the level found in the control animals. No additional measures were taken after day nine. This elevated luciferase activity in the first 72 hours correlates with adverse symptoms people may experience after vaccination.
The radioactivity study on the LNP shell found the highest levels in most tissues within eight to 48 hours after injection. Most of the LNP was concentrated in the liver. The report goes on to describe how long the lipids stay in the liver. One of the lipids (ALC-0315) may remain in the liver for four to five months when the data is extrapolated to humans. (pages 53-54)
Together, these two animal studies show that mRNA and the LNP shell can be found in tissues at peak concentrations within 72 hours.
Figure 1. Vaccination Adverse Reactions by Days Since Last Dose 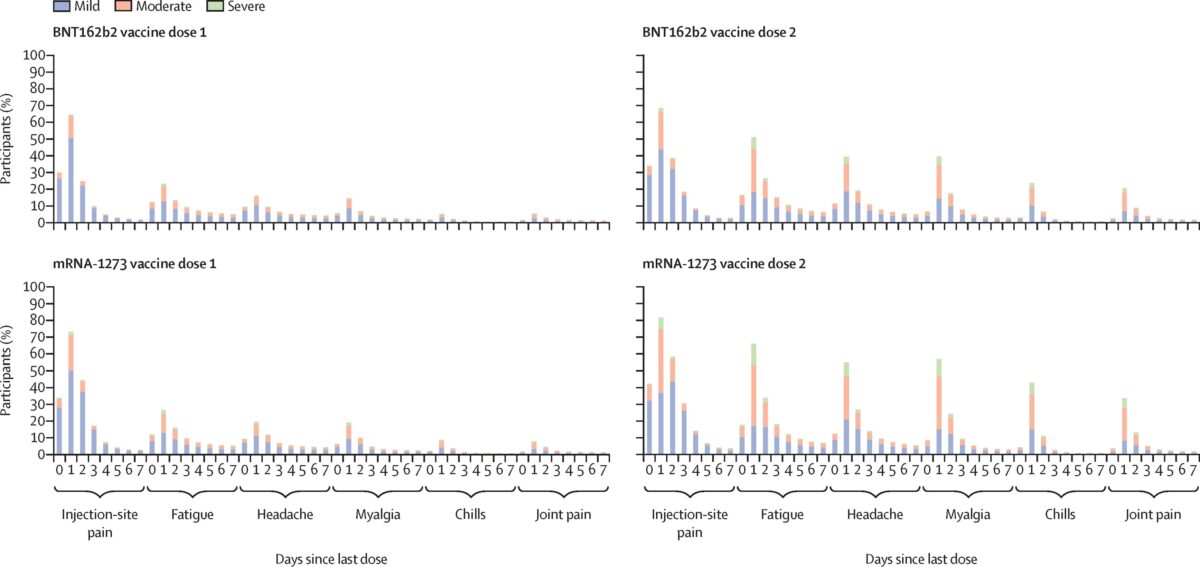 (The Lancet Infectious Diseases 2022 22802-812DOI: 10.1016/S1473-3099(22)00054-8)
(The Lancet Infectious Diseases 2022 22802-812DOI: 10.1016/S1473-3099(22)00054-8)
What Happens to the Spike Protein?
Once the vaccine LNP enters our cells and releases the mRNA, spike protein is produced and displayed on the surface of our cells. The mRNA code contains instructions to make the full-length spike protein, containing two subunits (S1 and S2). The immune system sees these cells displaying the spike protein and responds as if the virus had infected the cell.
When these cells are destroyed by the immune system, antibodies are made that bind to the spike protein. However, the spike protein, including its S1 subunit, can be released into the blood during this messy process of cell digestion by the immune system.
Circulation of the spike protein in the blood may explain some serious adverse events, such as myocarditis and other adverse events, including rare neurological issues which result from COVID-19 infection as well as BNT162b2 and mRNA-1273 vaccination.
For example, a study published in Circulation points out that “markedly elevated levels of full-length spike protein (33.9±22.4 pg/mL), unbound by antibodies, were detected in the plasma of individuals with post-vaccine myocarditis, whereas no free spike was detected in asymptomatic vaccinated control subjects (unpaired t-test; P<0.0001).” In other words, free spike protein may provide a clue about why some young people develop myocarditis following vaccination.
This study suggested that the difference was not caused by neutralizing antibodies in the myocarditis group, but was likely due to overactive innate immunity. In other words, having too many antibodies was not the cause of myocarditis. The authors suspect that another component of the immune system—innate immunity—might be involved.
Innate immunity is what helps the body fight off infection, even the first time it sees a new virus or bacteria. These innate “first responders” (inflammatory cytokines) need no training to identify foreign invaders. An overactive innate response is associated with allergies and may also be what triggers myocarditis.
Conversely, some authors have hypothesized that suppression of the natural innate immune response could explain some adverse events from the COVID-19 mRNA vaccine.
Because the active mRNA and the spike protein it encodes were never tested in animals or live tissue culture, there was no way to predict these issues. The FDA essentially allowed a product to be licensed without sufficient preclinical toxicity testing.
How Toxic Is the Lipid Nanoparticle Shell?
As the EMA reiterates, “No traditional pharmacokinetic or biodistribution studies have been performed with the vaccine candidate BNT162b2.” (page 45) The biodistribution studies are important because, as the EMA continues, “ALC-0315 and ALC-0159 are novel excipients, not previously used in an approved finished product within the EU.” These two novel “excipients” (ALC-0315 and ALC-0159) are the lipid nanoparticles used to create the LNP shell. They are new compounds, different from existing data on PEGylated compounds used in a wide variety of injected medications.
The EMA report further states that the half-life of the lipid ALC-0315 is quite long. (page 46) The term half-life means the amount of time it takes for half of the compound to be removed. On page 54, the EMA report clarifies that we might expect half of the ALC-0315 to be removed from the human body in about 20 to 30 days, and 95 percent to be removed in four to five months.
A separate deliberation summary (pdf) from the Japanese government’s Pharmaceutical Safety and Environmental Health Bureau (February 2021) reviewed all of the data prior to making a determination regarding authorization. The report showed effects on the liver which were “considered to be of little toxicological significance.” (page 20) However, the report also notes that “long-term repeated-dose toxicity of Comirnaty has not been evaluated” and therefore, the dosing regimen should be limited, and the use of lipids in the vaccine should not be considered a precedent. In other words, although PEGylated compounds have been used in medicine for years, there is limited information on their use as part of an LNP carrying a vaccine, thus no existing data to support repeated doses, such as boosters, beyond the original primary series.
The EMA concurred: “This [BNT162b2] vaccine contains two new components (cationic lipid ALC-0315 and PEGylated liquid ALC-0159) in the LNP, for which there is limited experience.” Given the long half-life of the ALC-0315 lipid and the toxicity of the PEG-lipid ALC-0159, the EMA acknowledged that while there are no immediate and obvious concerns for human use, there is also very limited data and the “current evidence is not definitive.”
“Regarding PEG-related toxicity which is known to depend on the dose, dose frequency, duration of treatment, and molecular weight of the PEG protein, immunogenicity is not expected to be an issue due to the low molecular weight of this PEG (<2KDa). The scientific data available at this stage do not raise noticeable concerns regarding immunogenicity or immunotoxicity of the PEG, but current evidence is not definitive.” (page 134)
The EMA notes that serious adverse events were twice as common in the vaccine group (21 percent) as in the placebo group (13 percent). The frequency was low overall (<1 percent) but the following system/organ/class adverse events were the most frequently reported: “General disorders and administration site conditions” (11.9 percent versus 2.9 percent), “musculoskeletal reactions” (5.5 percent versus 2.1 percent), and “nervous system disorders” (4.2 percent versus 2.1 percent).
Because the active ingredient (mRNA encoding spike protein) was not tested in these animal studies, these findings likely speak to the immunotoxicity of the LNP shell itself. Nevertheless, the EMA concluded that the benefits overall were positive enough to go forward given the protection afforded to the elderly and those with comorbidities.
Inflammation and Miscarriage Rates Noted in EMA Report
In repeat dose toxicity studies among rats given one dose per week for three weeks, joint and lymph node inflammation as well as changes in the bone marrow were observed. (page 49)
In reproductive toxicity tests (page 50), the report states: “There was an increase (~2x) of pre-implantation loss (9.77%, compared to control 4.09%) although this was within historical control data range (5.1%-11.5%).” In other words, although the miscarriage rate was twice as high in the vaccinated than in control animals, the rate was within the expected range based on previous studies. The same data can be found on page 55 of the Australian report.
Interestingly, the BNT162b1 candidate—one of Pfizer’s two vaccine candidates which coded for the receptor binding domain only, not the full-length spike—had a much lower pre-implantation loss rate (4.8 percent) than the vaccine eventually brought to market. The second model (BNT162b2) was chosen for global use because it had fewer side effects.
Some Types of Vision Loss Correlate with Vaccination
A new study in Nature confirms a “strong correlation between vaccination with an mRNA vaccine and retinal vascular occlusion.” The retina is part of the eye that receives light and converts it into nerve signals which are translated into vision in the brain. The retina is covered with tiny blood vessels, and when these become occluded (blocked) due to poor cardiovascular health or diabetes, vision is lost. The blockage in the vessels can be caused by swelling, spasms, poor blood flow into the vessels, and thromboembolism (clotting). Infection with SARS-CoV-2 is also linked to retinal occlusion.
Given the mounting evidence of vaccination causing occlusion, this study used medical records for approximately 6 million people to explore the long-term association between vaccination and occlusion. The authors matched 745,041 vaccinated and 3,874,458 unvaccinated people, resulting in a final comparison group of more than 500,000 individuals in each group.
Researchers found 415 cases among vaccinated people 18 to 64 years of age and 1108 cases among the vaccinated age 65 years or older. This represented a greater than threefold higher risk of retinal occlusion following vaccination within 12 weeks and a greater than twofold risk up to two years later compared to the unvaccinated. There was no difference in risk between mRNA vaccine brands (Pfizer versus Moderna) and the risk was elevated after both doses one and two. The risk was highest for the first two weeks and persisted for 12 weeks. The risk was similarly elevated across males and females as well as across race/ethnicity.
The authors of the study surmise that the similarity between spike proteins and human proteins may cause the blockage.
To summarize, these reports raise many concerning issues which we address in this series.
- The LNP capsule is dispersed throughout the body, mostly to the liver. Does it fall apart or stay in a capsule? How long does the LNP capsule persist in the body? Is the immune response to the LNP linked to post-vaccination blindness?
- The LNP can also cross the blood-brain barrier (BBB), as can the S1 subunit of the SARS-CoV-2 spike protein (in mice). What are the implications of the LNP and S1 subunits crossing the BBB?
- The lipid nanoparticle ALC-0315 has a long half-life (around six weeks in the liver). Does 95 percent of the lipid clear from the human body within four to five months as expected?
- The EMA states there is known immunotoxicity associated with polyethylene glycol (PEG) (page 134). This is the first time that PEG-lipid ALC-0159 has been used as a vaccine component in humans. What immune response is provoked by the PEG-lipid ALC-0159?
- How long does mRNA persist in the body? Does it stay in the capsule until it is released in cells? Does it fall out of the LNP capsule? What problems might mRNA cause if it circulates throughout the bloodstream? (Series Part 3)
- Free spike was found in myocarditis patients, but not controls. How long does the spike protein stay in the body? Where does it travel? How might the spike protein or its S1 subunit cause myocarditis or other adverse events which may include neurologic issues? (Series Part 4)
- The EMA report also noted impurities in the vaccine doses produced using the commercial manufacturing process which were not found in the vials used in the clinical trials. These impurities include RNA fragments which may code for unexpected proteins, potentially causing adverse reactions, including allergic reactions, which we will discuss later in this series. The latter demonstrates an uncanny predominance in females raising the need for tailored risk assessment along yet another parameter. (Series Part 5)
- What is causing effects on peripheral nerves such as Bell’s Palsy? What is the latest research describing neurologic, cardiac, autoimmune, and reproductive adverse events? Is there anything people can do to reduce the risk of a future adverse event?
The adverse events noted by the EMA in January 2021 suggest that more thorough animal testing and additional biodistribution and safety studies in humans should have been performed before licensing these products. In addition, the EMA report noted that differences in batches were found. Additional reports were requested from the manufacturer. Where is the public communication regarding updates on these issues? Why did the FDA not apply stricter mRNA “genetic therapy” standards to the regulation of mRNA vaccines? In other words, why were vaccines given a special pass when they were using the same technology platform?
Required studies could have been performed even within the compressed timeframe. Furthermore, given the massive earnings these products have garnered from global distribution, why are the post-marketing studies not accelerated? As a final example of this lagging regulatory framework, the FDA requested post-marketing surveillance does not require submission of reports on the incidence and natural course of vaccine myocarditis until September 2024.
This article is part of the Vaccine series.
Embalmers Have Been Finding Numerous Long, Fibrous Clots That Lack Post-Mortem Characteristics
Pulling Back the Curtain: mRNA Lipid Nanoparticle Design Created Potential for Clotting and Triggering Immune OverdriveReferences
Addgene. Molecular Biology Reference.
Alana F Ogata, Chi-An Cheng, Michaël Desjardins, Yasmeen Senussi, Amy C Sherman, Megan Powell, Lewis Novack, Salena Von, Xiaofang Li, Lindsey R Baden, David R Walt, Circulating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients, Clinical Infectious Diseases, Volume 74, Issue 4, 15 February 2022, Pages 715–718.
Aldén M, Olofsson Falla F, Yang D, Barghouth M, Luan C, Rasmussen M, De Marinis Y. Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line. Curr Issues Mol Biol. 2022 Feb 25;44(3):1115-1126. doi: 10.3390/cimb44030073. PMID: 35723296; PMCID: PMC8946961.
Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine—United States, December 14–23, 2020. MMWR Morb Mortal Wkly Rep 2021;70:46–51. DOI.
Anderson EJ, Rouphael NG, Widge AT, et al. Safety and Immunogenicity of SARS-CoV-2 mRNA-1273 Vaccine in Older Adults N Engl J Med 2020; 383:2427-2438.
Anderson S. CBER Plans for Monitoring COVID-19 Vaccine Safety and Effectiveness. October 20, 2020. Accessed 3/20/23.
Angeli F, Spanevello A, Reboldi G, Visca D, Verdecchia P. SARS-CoV-2 vaccines: Lights and Shadows. Eur J Intern Med. 2021 Jun;88:1-8. doi: 10.1016/j.ejim.2021.04.019. Epub 2021 Apr 30. PMID: 33966930; PMCID: PMC8084611.
Baker, A. T., Boyd, R. J., Sarkar, D., Teijeira-Crespo, A., Chan, C. K., Bates, E., Waraich, K., Vant, J., Wilson, E., Truong, C. D., Lipka-Lloyd, M., Fromme, P., Vermaas, J., Williams, D., Machiesky, L., Heurich, M., Nagalo, B. M., Coughlan, L., Umlauf, S., Chiu, P. L., … Borad, M. J. (2021). ChAdOx1 interacts with CAR and PF4 with implications for thrombosis with thrombocytopenia syndrome. Science Advances. 7(49), eabl8213.
Baumeier C, Aleshcheva G, Harms D, Gross U, Hamm C, Assmus B, Westenfeld R, Kelm M, Rammos S, Wenzel P, Münzel T, Elsässer A, Gailani M, Perings C, Bourakkadi A, Flesch M, Kempf T, Bauersachs J, Escher F, Schultheiss H-P. Intramyocardial Inflammation after COVID-19 Vaccination: An Endomyocardial Biopsy-Proven Case Series. International Journal of Molecular Sciences. 2022; 23(13):6940.
Bloom, K., van den Berg, F. & Arbuthnot, P. Self-amplifying RNA vaccines for infectious diseases. Gene Ther 28, 117–129 (2021).
Chauhan, H., Mohapatra, S., Munt, D.J. et al. Physical-Chemical Characterization and Formulation Considerations for Solid Lipid Nanoparticles. AAPS PharmSciTech 17, 640–651 (2016).
Chui CSL, Fan M, Wan EYF, et al. Thromboembolic events and hemorrhagic stroke after mRNA (BNT162b2) and inactivated (CoronaVac) covid-19 vaccination: A self-controlled case series study. Lancet. 2022;(50).
Dag Berild J, Bergstad Larsen V, Myrup Thiesson E, et al. Analysis of Thromboembolic and Thrombocytopenic Events After the AZD1222, BNT162b2, and MRNA-1273 COVID-19 Vaccines in 3 Nordic Countries. JAMA Netw Open. 2022;5(6):e2217375. doi:10.1001/jamanetworkopen.2022.17375.
daSilva RL. Viral-associated thrombotic microangiopathies. Hematology/Oncology and Stem Cell Therapy. 2011:4(2):51-59.
De A, Ko YT. Why mRNA-ionizable LNPs formulations are so short-lived: causes and way-out. Expert Opin Drug Deliv. 2023 Feb;20(2):175-187. doi: 10.1080/17425247.2023.2162876. Epub 2023 Jan 1. PMID: 36588456.
Ehaideb, S.N., Abdullah, M.L., Abuyassin, B. et al. Evidence of a wide gap between COVID-19 in humans and animal models: a systematic review. Crit Care 24, 594 (2020).
European Medicines Agency Assessment Report Comirnaty (pdf)
Faizullin D, Valiullina Y, Salnikov V, Zuev Y. Direct interaction of fibrinogen with lipid microparticles modulates clotting kinetics and clot structure. Nanomedicine. 2020 Jan;23:102098. doi: 10.1016/j.nano.2019.102098. Epub 2019 Oct 23. PMID: 31655206.
FDA. Considerations for Human Radiolabeled Mass Balance Studies—Guidance for Industry. May, 2022.
FDA. Development and Licensure of Vaccines to Prevent COVID-19.
FDA-CBER-2021-5683-0013962 approved on: 09-Nov-2020. A Tissue Distribution Study of a [3H]-Labeled Lipid Nanoparticle-mRNA Formulation Containing ALC-0315 and ALC-0159 Following Intramuscular Administration in Wistar Han Rats. (pdf) FINAL REPORT Test Facility Study No. 185350 Sponsor Reference No. ALC-NC-0552.
Fertig TE, Chitoiu L, Marta DS, Ionescu VS, Cismasiu VB, Radu E, Angheluta G, Dobre M, Serbanescu A, Hinescu ME, Gherghiceanu M. Vaccine mRNA Can Be Detected in Blood at 15 Days Post-Vaccination. Biomedicines. 2022 Jun 28;10(7):1538. doi: 10.3390/biomedicines10071538. PMID: 35884842; PMCID: PMC9313234.
Grobbelaar LM et al. SARS-CoV-2 spike protein S1 induces fibrin(ogen) resistant to fibrinolysis: implications for microclot formation in COVID-19 Biosci Rep (2021) 41 (8): BSR20210611.
Hou, X., Zaks, T., Langer, R. et al. Lipid nanoparticles for mRNA delivery. Nat Rev Mater 6, 1078–1094 (2021).
Iaboni A, Jindal N, Betschel SD, Song C. Second-dose mRNA COVID-19 vaccine safety in patients with immediate reactions after the first dose: A case series. Journal of Allergy and Clinical Immunology: Global. 2022;1(3): 172-174.
Let’s talk about lipid nanoparticles. Nat Rev Mater 6, 99 (2021).
Li, JX., Wang, YH., Bair, H. et al. Risk assessment of retinal vascular occlusion after COVID-19 vaccination. npj Vaccines 8, 64 (2023).
Michieletto, D., Lusic, M., Marenduzzo, D. et al. Physical principles of retroviral integration in the human genome. Nat Commun 10, 575 (2019).
Moghimi, S. M., & Simberg, D. (2022). Pro-inflammatory concerns with lipid nanoparticles. Molecular therapy: The Journal of the American Society of Gene Therapy, 30(6), 2109–2110.
Naturally Inspired Podcast. Jessica Rose Ph.D.—VAERS, Data And Truth
Ohlson J. Plasmid manufacture is the bottleneck of the genetic medicine revolution. Drug Discov Today. 2020 Oct 16;25(11):1891–3. doi: 10.1016/j.drudis.2020.09.040. Epub ahead of print. PMID: 33075470; PMCID: PMC7564888.
Perico L, Marina Morigi M, Galbusera M, et al. SARS-CoV-2 Spike Protein 1 Activates Microvascular Endothelial Cells and Complement System Leading to Platelet Aggregation. Front. Immunol. 2022
Qin, S., Tang, X., Chen, Y. et al. mRNA-based therapeutics: powerful and versatile tools to combat diseases. Sig Transduct Target Ther 7, 166 (2022).
Rafati A, Pasebani Y, Jameie M, et al. Association of SARS-CoV-2 Vaccination or Infection With Bell Palsy: A Systematic Review and Meta-analysis. JAMA Otolaryngol Head Neck Surg. Published online April 27, 2023. doi:10.1001/jamaoto.2023.0160
Rhea EM, Logsdon AF, Hansen KM, Williams LM, Reed MJ, Baumann KK, Holden SJ, Raber J, Banks WA, Erickson MA. The S1 protein of SARS-CoV-2 crosses the blood-brain barrier in mice. Nat Neurosci. 2021 Mar;24(3):368-378. doi: 10.1038/s41593-020-00771-8. Epub 2020 Dec 16. PMID: 33328624; PMCID: PMC8793077.
Röltgen K, Nielsen SCA, Silva O. Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Cell 2022;185(6):1025-1040.
Rosenblum HG, Gee J, Liu R, et al. Safety of mRNA vaccines administered during the initial 6 months of the US COVID-19 vaccination programme: an observational study of reports to the Vaccine Adverse Event Reporting System and v-safe. Lancet Infectious Diseases. 2022;22(6):802-812.
Schmeling, M, Manniche, V, Hansen, PR. Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine. Eur J Clin Invest. 2023; 00:e13998. doi:10.1111/eci.13998
Srinivasan M, Thangaraj SR, Arzoun H. Gene Therapy – Can it Cure Type 1 Diabetes? Cureus. 2021 Dec 19;13(12):e20516. doi: 10.7759/cureus.20516. PMID: 35004071; PMCID: PMC8723777.
Trougakos IP, Terpos E, Alexopoulos H, et al. Adverse effects of COVID-19 mRNA vaccines: the spike hypothesis. Cell 2022;28(7): P542-554.
Vervaeke P, Borgos SE, Sanders NN, Combes F. Regulatory guidelines and preclinical tools to study the biodistribution of RNA therapeutics. Adv Drug Deliv Rev. 2022 May;184:114236. doi: 10.1016/j.addr.2022.114236. Epub 2022 Mar 26. PMID: 35351470; PMCID: PMC8957368.
Wong DWL, Klinkhammer BM, Djudjaj S, Villwock S, Timm MC, Buhl EM, Wucherpfennig S, Cacchi C, Braunschweig T, Knüchel-Clarke R, Jonigk D, Werlein C, Bülow RD, Dahl E, von Stillfried S, Boor P. Multisystemic Cellular Tropism of SARS-CoV-2 in Autopsies of COVID-19 Patients. Cells. 2021 Jul 27;10(8):1900. doi: 10.3390/cells10081900. PMID: 34440669; PMCID: PMC8394956.
Yonker LM, Swank Z, Bartsch YC, et al. Circulating Spike Protein Detected in Post–COVID-19 mRNA Vaccine Myocarditis. Circulation. 2023:147(11).
About the Authors:
Allison Krug is an epidemiologist and program manager with experience leading population health programs. She's the lead author of the first stratified risk-benefit analysis of mRNA vaccination among adolescents and editor for 400+ research manuscripts published in high impact factor, peer-reviewed journals. She's also the founder and CEO of Artemis Biomedical Communications, LLC.
Dr. Duriseti is a clinical associate professor and physician-scientist at Stanford University. He received his M.D. from the University of Michigan and his medical training and Ph.D. in Computational Decision Modeling from Stanford University. He has practiced in clinical Emergency Medicine in both community and academic settings for over 22 years.
Reposted from: https://www.theepochtimes.com/health/health-implications-of-poor-covid-19-mrna-testing-miscarriage-vision-loss-immunotoxicity_5201116.html







.png)
Comments
Post a Comment