Long COVID Treatment Protocol (2023)
As of May 8, 2023, federal data published by the US CDC found that 15.1% (National Estimate) of adults who previously had a COVID-19 infection are currently experiencing symptoms of long COVID. Females tend to have a relatively higher risk as compared to males.
The survey’s results mean that over 18 million adult Americans are currently experiencing symptoms of long COVID and 15 million have problems performing daily activities because of it.
The data helps to round out the picture of long COVID, a condition the CDC defines as a “wide range of new, returning or ongoing health problems people can experience four or more weeks after first being infected with the virus that causes COVID-19.”
Update: Outpatient treatment with metformin reduced long COVID incidence by about 41%, compared with placebo (The Lancet 2023)
When the COVID-19 pandemic first stormed the globe three years ago, the coronavirus was believed to be largely a respiratory ailment that also damaged the cells that line the blood vessels. But research is now showing that the virus can spread throughout the body and remain lodged in organs. This might offer one clue about the lingering phenomenon of “long covid” and suggest why it will remain a serious problem for individuals and the heath-care system for some time to come. The entire world will have to prepare for a legacy of long-covid sufferers.
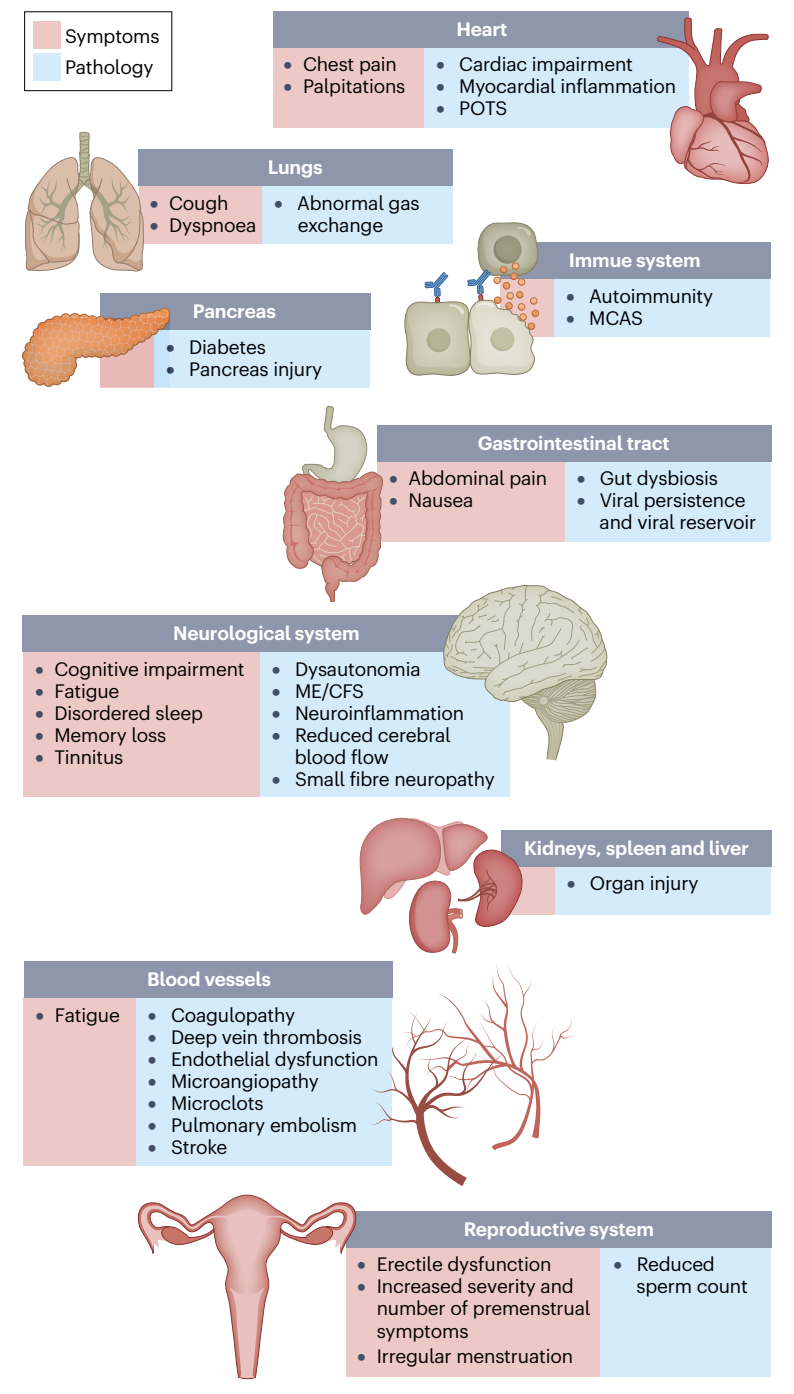
A study, published in Nature in January 2023, pointed out that long-covid symptoms can crop up in the heart, lungs, immune system, pancreas, gastrointestinal tract, neurological system, kidneys, spleen and liver, blood vessels and reproductive system.
If you’re still coping with symptoms three months or more after being infected with COVID-19, you’re considered a COVID long-hauler. Post-COVID recovery clinics are being launched nationwide to address this still-growing need. Multiple studies have shown that the SARS-CoV-2 spike protein is a highly toxic and inflammatory protein, capable of causing pathologies in its hosts.
The presence of spike protein has been strongly linked with long COVID. Studies have shown that spike proteins are often present in symptomatic patients, sometimes even months after infections.
As we learn more about post-COVID syndrome, however, the definition has been refined to be more accurate and useful:
- Subacute or ongoing COVID-19 (post-acute COVID-19 syndrome): symptoms continuing beyond four weeks from acute infection, up to 12 weeks.
- Post-acute sequelae of COVID-19 (PASC): symptoms persisting beyond the four weeks after acute infection.
- Post-COVID-19 syndrome (long COVID, long-hauler’s syndrome): chronic ongoing COVID-19 symptoms beyond 12 weeks from acute infection.
With 200-plus symptoms linked to long COVID, treatment starts by pinpointing specific medical conditions and referring patients to the right clinicians. These might be lung specialists, heart specialists or brain rehabilitation experts. Patients need a carefully designed but flexible long haul COVID treatment protocol tailored to their particular symptoms and needs.
Understanding long haulers syndrome and the possible treatments is a vast and dynamic subject. Given the lack of specific treatments of long-haul COVID-19 syndrome, we have compiled and curated relevant and useful information and evidence from various sources about long haulers syndrome. As with most of our articles, the information will evolve as more clinical evidence accumulates.
Long COVID Symptoms
According to CDC, post-COVID Conditions are referred to by a wide range of names, including:
- Long COVID
- Post-acute COVID-19
- Long-term effects of COVID
- Post-acute COVID syndrome
- Chronic COVID
- Long-haul COVID
- Late sequelae
- Post-acute sequelae of SARS-COV-2 infection (PASC)
While the CDC tracks the prevalence of 26 common post-COVID conditions affecting a significant body system, more than 50 long-term effects, particularly fatigue, headache, attention disorders, shortness of breath and hair shedding, are now attributed to long-hauler’s syndrome (R).
An international study showed that fatigue is the most common long-hauler’s syndrome, affecting 80% of all patients. Post-exertional malaise affects 73%, cognitive dysfunction affects 58%, sensorimotor symptoms such as loss of smell affect 56%, headache affects 54%, and memory issues affect 51% (R). A year after infection, common persistent symptoms include fatigue (reported by 82% of patients), brain fog (written by 67%), and headache (reported by 60%) (R).
Clinical signs and symptoms can be grouped in the following clusters. The reason for this grouping is to allow organ specific targeted therapy/individualized therapy.
1. Respiratory: shortness of breath, congestion, persistent cough, etc.
2. Neurological/psychiatric: brain fog, malaise, tiredness, headaches, migraines, depression, inability to focus/concentrate, altered cognition, insomnia, vertigo, panic attacks, tinnitus, anosmia, phantom smells, parosmia etc.
3. Musculoskeletal: myalgias, fatigue, weakness, joint pains, inability to exercise, post-exertional malaise, inability to perform normal activities of daily life (ADL’s), muscle mass loss
4. Cardiovascular: Palpitations, arrhythmias, Raynaud like syndrome, hypotension, and tachycardia on exertion.
5. Autonomic: Postural tachycardia syndrome (POTs), abnormal sweating.
6. GIT disturbance: Anorexia, diarrhea, bloating, vomiting, nausea, etc.
7. Dermatologic: Itching, rashes, dermatographia, hair loss.
8. Mucus membranes: Running nose, sneezing, Burning and itchy eyes.
10. Endocrine dysfunction: adrenal gland dysfunction., thyroid dysfunction, estrogen and progesterone dysfunction, testosterone dysfunction.
 |
| Source: Davis, H.E., McCorkell, L., Vogel, J.M. et al. Long COVID: major findings, mechanisms and recommendations. Nature Rev Microbiol (2023) |
If the symptoms include major shortness of breath, cough with blood in it or pain on one side when you take a deep breath, it could be due to a late pulmonary embolism or a blood clot going to the lungs. Please visit your medical doctor or the nearest 24-hr medical emergency center immediately.
FLCCC I-Recover Protocol
The FLCCC (Front Line COVID-19 Critical Care Alliance) was formed by leading critical care specialists in March 2020, at the beginning of the Coronavirus pandemic, dedicated to developing highly effective treatment protocols to prevent the transmission of COVID-19 and to improve the outcomes for patients ill with the disease.Though there are many long haul COVID treatment protocols out there, we consider and recommend the I-Recover for Long Haul as one of the best.
Due to the marked overlap between long COVID and post-vaccine syndrome, please refer to the I-RECOVER Post-Vaccine Treatment protocol below for detailed treatment strategies.
Note that there are two post-vaccine protocols, one to treat post vaccine injury (I-Recover Post Vaccine) and the other to prevent post vaccine injury (I-Prevent Post Vaccine).
Patients with post-vaccine syndrome should do whatever they can to prevent themselves from getting COVID-19. This may include a preventative protocol (see I-PREVENT) or early treatment in the event you do contract the virus or suspect infection (see I-CARE). COVID-19 will likely exacerbate the symptoms of vaccine injury.
Once a patient has shown improvement, the various interventions should be reduced or stopped one at a time. A less intensive maintenance approach is then suggested.
The core problem in post-vaccine syndrome is long-lasting “immune dysregulation.” The most important treatment goal is to help the body restore a healthy immune system — in other words, to let the body heal itself. Our recommended treatment strategy involves two major approaches:
There are also some important cautions and contraindications that should be carefully reviewed within the more comprehensive and detailed document called “An Approach to Managing Post-Vaccine Syndrome” and which should be discussed with a qualified provider as well.
It appears that vaccine-injured patients can be grouped into two categories: i) ivermectin responders and ii) ivermectin non-responders. This distinction is important, as the latter are more difficult to treat and require more aggressive therapy.
For ivermectin responders, prolonged and chronic daily treatment is often necessary to support their recovery. In many, if the daily ivermectin is discontinued worsening symptoms often recur within days.
The I-Recover protocol has been updated and below is their latest version (Feb 10, 2023).
Treatment must be individualized according to each patient’s presenting symptoms and disease syndromes. It is likely that not all patients will respond equally to the same intervention; a particular intervention may be life-saving for one patient and totally ineffective for another. Early treatment is essential; it is likely that the response to treatment will be attenuated when treatment is delayed.
Patients with post-vaccine syndrome should do whatever they can to prevent themselves from getting COVID-19. This may include a preventative protocol (see I-PREVENT) or early treatment in the event you do contract the virus or suspect infection (see I-CARE). COVID-19 will likely exacerbate the symptoms of vaccine injury.
Once a patient has shown improvement, the various interventions should be reduced or stopped one at a time. A less intensive maintenance approach is then suggested.
The core problem in post-vaccine syndrome is long-lasting “immune dysregulation.” The most important treatment goal is to help the body restore a healthy immune system — in other words, to let the body heal itself. Our recommended treatment strategy involves two major approaches:
- Promote autophagy to help rid the cells of the spike protein
- Use interventions that limit the toxicity/pathogenicity of the spike protein
First Line Therapies
(Not symptom specific; listed in order of importance)- Intermittent daily fasting or periodic daily fasts
- Ivermectin (Stone 2022)
- Moderating physical activity
- Low-dose naltrexone
- Nattokinase (Tanikawa 2022)
- Aspirin
- Melatonin
- Magnesium
- Methylene blue
- Sunlight and Photobiomodulation (Red Light Therapy)
- Resveratrol
Second-Line Therapies
(Listed in order of importance)
- Probiotics/Prebiotics (Lau 2023)
- Vitamin D (with Vitamin K2)
- N-acetyl cysteine (NAC)
- Cardio Miracle™ and L-arginine/L-citrulline supplements
- Omega-3 fatty acids
- Sildenafil (with or without L-arginine and L-citrulline)
- Nigella sativa
- Vitamin C
- Spermidine
- Non-invasive brain stimulation
- Intravenous Vitamin C
- Behavioral modification, relaxation therapy, mindfulness therapy, and psychological support
Third Line Therapies
- Hyperbaric oxygen therapy (HBOT)
- Low Magnitude Mechanical Stimulation
- “Mitochondrial energy optimizer” with pyrroloquinoline quinone, glycophospholipids, CoQ10, NADH, and other nutrients (e.g., Life Extension Energy Optimizer, Restorative Solutions Mitochondrial Nutrition PQQ, Researched Nutritionals ATP 360® and ATP Fuel® and PureEncapsulations Mitochondria-ATP)
- Hydroxychloroquine
- Low-dose corticosteroid
Warning (anesthesia and surgery):
Patients should notify their anesthesia team if using the following medications and/or nutraceuticals, as they can increase the risk of Serotonin syndrome (SS) with opioid administration:
- Methylene blue
- Curcumin
- Nigella Sativa
- Selective Serotonin Reuptake Inhibitors (SSRIs)
About Ivermectin
Ivermectin is a well-known, FDA-approved drug that has been used successfully around the world for more than four decades. One of the safest drugs known, it is on the WHO’s list of essential medicines, has been given over 3.7 billion times, and won the Nobel Prize for its global and historic impacts in eradicating endemic parasitic infections in many parts of the world.
Review the totality of supporting evidence for ivermectin: https://c19ivm.org.
It is likely that ivermectin and intermittent fasting act synergistically to rid the body of the spike protein.It appears that vaccine-injured patients can be grouped into two categories: i) ivermectin responders and ii) ivermectin non-responders. This distinction is important, as the latter are more difficult to treat and require more aggressive therapy.
For ivermectin responders, prolonged and chronic daily treatment is often necessary to support their recovery. In many, if the daily ivermectin is discontinued worsening symptoms often recur within days.
Ivermectin is best taken with or just following a meal, for greater absorption.
Moving Forward
One of the pandemic’s few bright spots is the way it’s accelerated telehealth services. Patients now can have unprecedented access to a broad range of healthcare providers across the nation.
Find healthcare providers:
- List of Doctors that will prescribe Ivermectin and Hydroxychloroquine
- List of Pharmacies that will fill Ivermectin
- www.ifm.org/find-a-practitioner (Functional Medicine)
- Post-COVID Care Centers (PCCC) by Survivor Corps
Read more articles related to Long COVID > Long COVID series








Comments
Post a Comment