Early Flu Treatment with Oseltamivir Associated with Reduced Mortality - Dr Peter McCullough
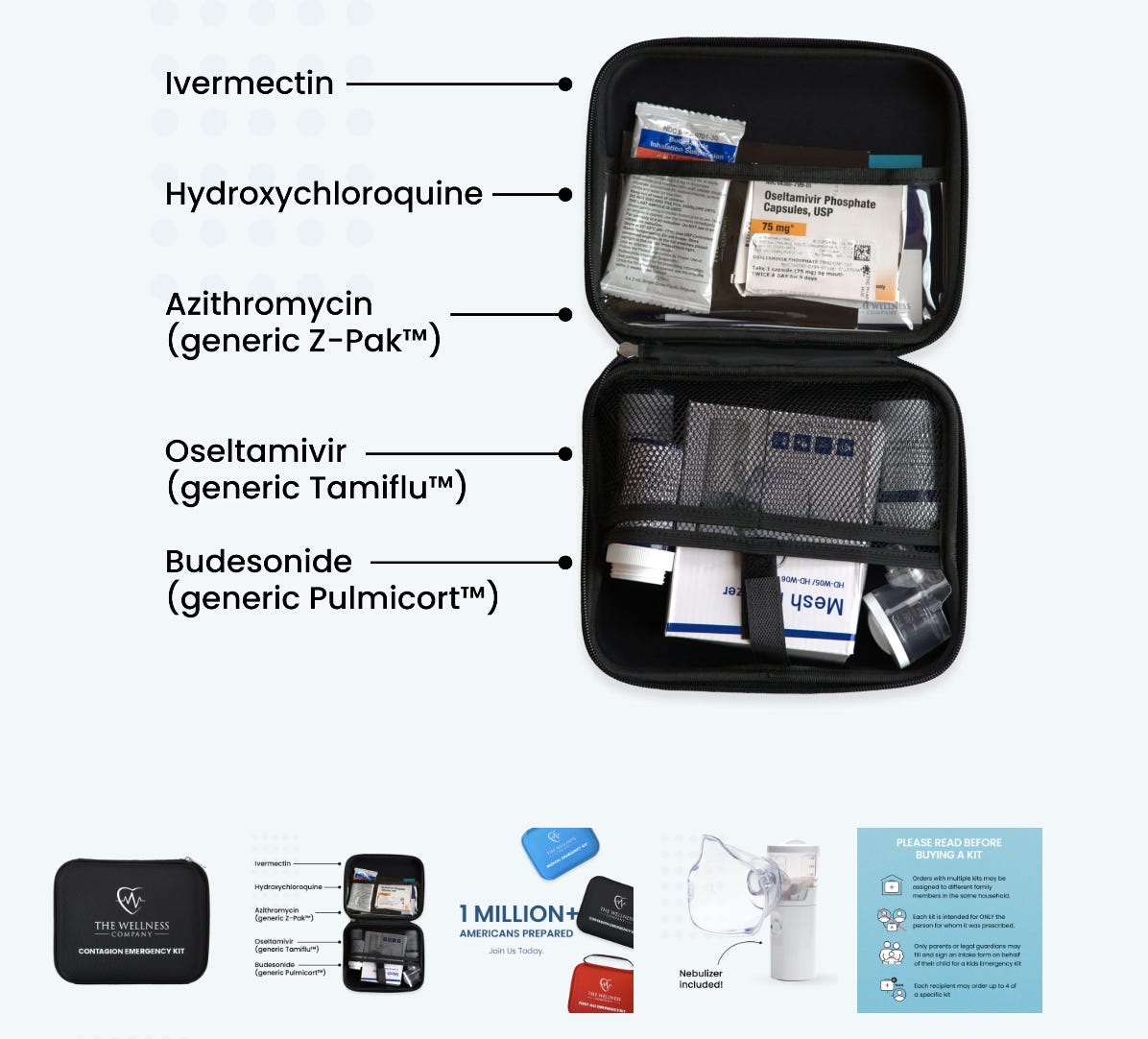
Many colleagues challenged the inclusion of oseltamivir in the Contagion Emergency Kits offered by The Wellness Company. It has always been my clinical understanding that viral replication in any upper respiratory illness occurs early, and hence later administration captured in studies will bias to the null effect.
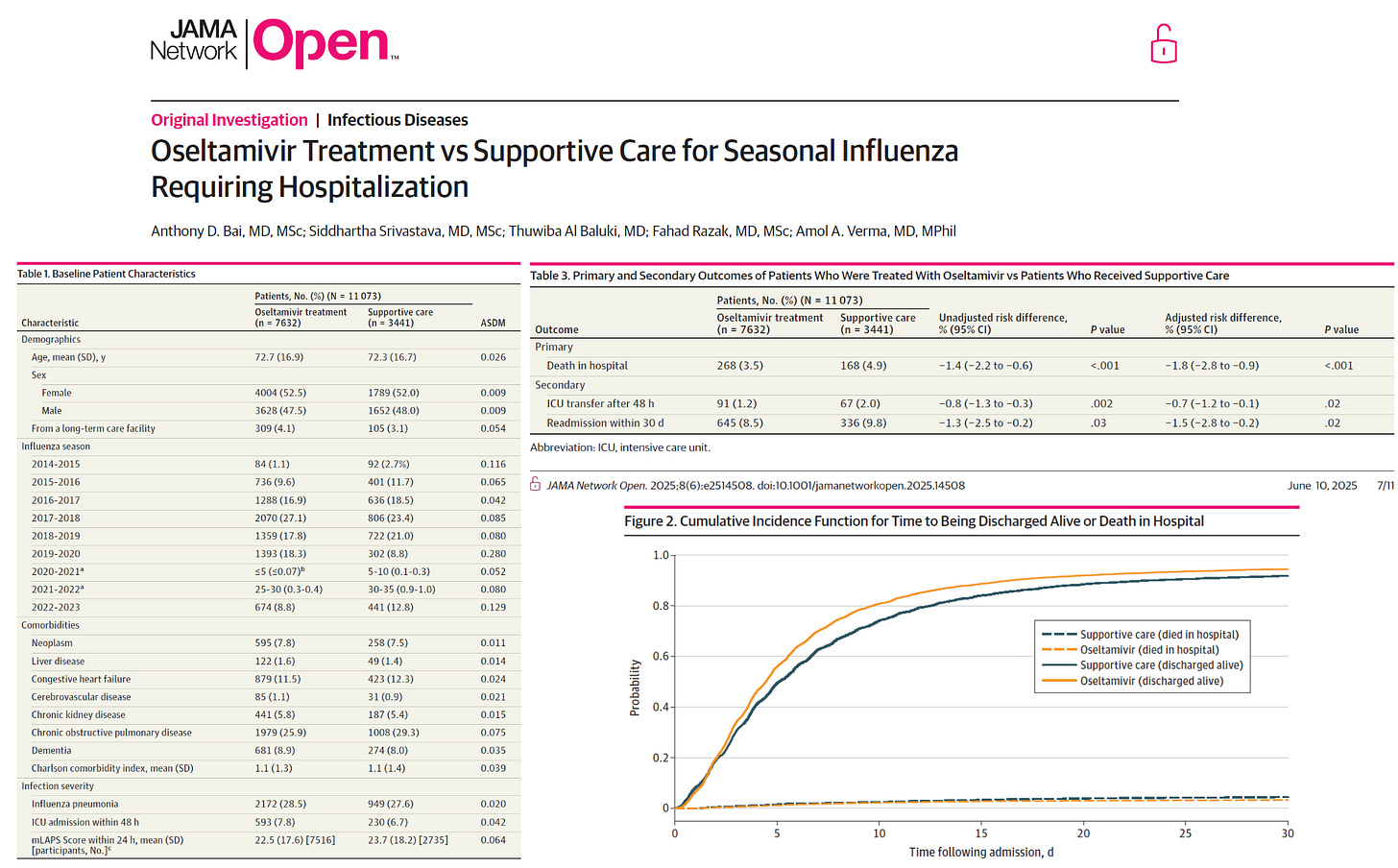
Bai et al (JAMA 2025) studied a large group of elderly Canadians hospitalized with influenza, of whom 69% received oseltamivir.
Of 11 073 patients (mean [SD] age, 72.6 [16.8] years; 5793 female [52.3%]), there were 7632 patients (68.9%) and 3441 patients (31.1%) in the oseltamivir and supportive care groups, respectively. In hospital, 268 patients (3.5%) and 168 patients (4.9%) in the oseltamivir and supportive care groups died, respectively, with an adjusted risk difference of −1.8% (95% CI, −2.8% to −0.9%; P < .001). The oseltamivir treatment group was more likely to be discharged alive (adjusted subdistribution hazard ratio, 1.20; 95% CI, 1.15 to 1.25; P < .001). After discharge, 645 patients (8.5%) and 336 patients (9.8%) were readmitted in the oseltamivir and supportive care groups, respectively, with an adjusted risk difference of −1.5% (95% CI, −2.8% to −0.2%; P = .02).
I can tell you that a 28.6% reduction in mortality with oseltamivir is clinically meaningful particularly considering hospitalized patients receive other supportive care including intravenous fluids, secondary antibiotics, and oxygen etc.
Bai et al (JAMA 2025) studied a large group of elderly Canadians hospitalized with influenza, of whom 69% received oseltamivir.
Of 11 073 patients (mean [SD] age, 72.6 [16.8] years; 5793 female [52.3%]), there were 7632 patients (68.9%) and 3441 patients (31.1%) in the oseltamivir and supportive care groups, respectively. In hospital, 268 patients (3.5%) and 168 patients (4.9%) in the oseltamivir and supportive care groups died, respectively, with an adjusted risk difference of −1.8% (95% CI, −2.8% to −0.9%; P < .001). The oseltamivir treatment group was more likely to be discharged alive (adjusted subdistribution hazard ratio, 1.20; 95% CI, 1.15 to 1.25; P < .001). After discharge, 645 patients (8.5%) and 336 patients (9.8%) were readmitted in the oseltamivir and supportive care groups, respectively, with an adjusted risk difference of −1.5% (95% CI, −2.8% to −0.2%; P = .02).
I can tell you that a 28.6% reduction in mortality with oseltamivir is clinically meaningful particularly considering hospitalized patients receive other supportive care including intravenous fluids, secondary antibiotics, and oxygen etc.








Comments
Post a Comment