What's driving turbo cancers and autoimmune flare-ups?
Pointed or pointless?
The public is understandably confused. On the one hand, major scientific journals, news outlets and authorities have used, and continue to use, superlatives to describe C-XX genetic vaccines. The journal Science called the results of a Moderna trial “absolutely remarkable”, the Washington Post referred to them as “an extraordinary success story”, BuzzFeed claimed the vaccines “work way better than we had ever expected”, while the US Centers for Disease Control and Prevention (CDC), the UK National Health Service (NHS) and other authorities continue to cite the mantra used for all approved vaccines, referring them as “safe and effective” (here and here, respectively).
Conflicting information about an uncertain and unpredictable interaction
Yet, on the other hand, the scientific literature is increasingly awash with articles that suggest something quite different.
The CDC is still telling US citizens to “stay up to date” with their shots, yet a preprint study released in June shows that Cleveland Clinic staff who weren’t “up-to-date” with their C-XX shots fared better against C-XX than those who were.
As early as 2021, as indicated in an article in Nature Medicine, “viral variants began to stack up” only after the vaccines were rolled out. An article published in Frontiers in Immunology in early 2022 details the multiple immune escape strategies used by the virus both following infection and vaccination.
Then there’s people’s individual experiences, with many who have been heavily vaccinated not experiencing good outcomes, either in relation to C-XX disease, a concern noted in the recently published Cleveland Clinic study – but also in relation to other diseases or conditions, cancer and autoimmune diseases included.
Emergency over – or not?
For most people, the C-XX crisis is over. That’s largely a consequence of the World Health Organization’s declaration in May this year that the “public health emergency” was no longer.
There are at least two reasons it is likely wrong to think that the C-XX drama is behind us.
The first is that the virus is still very much out there, circulating to its non-existent heart’s content. While it remains at large, it is susceptible to natural selection of immune escape variants. Secondly, it seems authorities have no inclination to sideline C-XX shots. By contrast, they want to keep using them, and no doubt will use any obvious waves of C-XX disease as we progress towards the northern winter to justify more vaccination.
There is no shortage of acclaimed ‘experts’ who can confirm for you that SARS-CoV-2 hasn’t transitioned to an endemic, seasonal pattern, as naturally-occurring respiratory viruses typically do after the pandemic phase. It’s still very much around as you may have noticed in you own circles — it’s just not being surveilled with the same intensity via C-XX testing stations dotted around each and almost every industrialised country. Ditching the nationwide testing programmes wasn’t just seen as a waste of resources, it might also have been recognised that its continuation would dent people’s faith in the genetic vaccines, a reputation the establishment seems very keen to protect.
An article just published in STAT included feedback from numerous acknowledged experts in the field, ones aligned with the mainstream scientific establishment, including Michael Osterholm, director of the University of Minnesota’s Center for Infectious Disease Research and Policy. Most of the experts interviewed confirm that the virus has yet to achieve true endemicity and seasonal patterns.
This equates with the lack of understanding of how population-level immunity shapes the evolutionary dynamics of the virus, a phenomenon that is greatly complicated by the genetic vaccination programme. In fact, it is this poor insight that remains one of the most defining characteristics of a virus put under immune selection pressure after its release on human populations over three years ago, making a mockery of much of the predictive modelling that has been undertaken to-date.
Conflicting information doesn’t just create confusion. It creates cognitive dissonance. That’s an uncomfortable and unsettling feeling – and it drives people to find, and latch onto, what feels to them like a coherent, trusted view. This causes division. Some still have trust in the authorities and the scientific establishment that remain steadfastly on the ‘vaccines-are-our-best-fix’ podium. Others of us cannot support this view, seeing it as incoherent, both scientifically and experientially.
Many of us have lost trust in the scientific establishment, full stop. See here and here for our reasons why. Any trust that we might have had prior to the C-XX crisis has since evaporated, largely because of the way the crisis, and information relating to it, was handled. That includes the mass censorship of dissenting scientific views.
Given the social nature of human beings, and our desire to align with those we trust, if we are repelled by one group we distrust – such as the scientific establishment responsible for our ‘C-XX worldview’ – we find ourselves being attracted to others with whom we see reason to trust.
GVB – dedicated to better understanding the uncertainty
It is in this vein that I get to the main purpose of the present piece. It is to introduce you to a new article by a person who has been something of an icon for many of us who have been attempting to grapple with the complexity of our immune systems’ dance with the ever-changing SARS-CoV-2 virus. Changes that have been undoubtedly amplified greatly by the global C-XX vaccine programme. The person to whom I refer is of course immunologist and vaccinologist, Geert Vanden Bossche DVM, PhD, a person I admire greatly both for his scientific rigour and his resolve, but also for his bravery in the face of the monolith we might refer to as the scientific-medical-industrial complex. I am also humbled to regard Geert as both an ally and a friend.
Before offering you a précis of Geert’s latest thoughts based on extensive evidence, all compiled in a brand new report, I also want to highlight that Geert has dedicated this report, that we have designed into a standalone publication, to John Heathco, a computer engineer and self-confessed “health & wellness junkie”, who died suddenly and tragically in June, along with his girlfriend.
On June 13, John and his girlfriend, Abby Lutz, died tragically overnight while in a 5-star hotel, on holiday in Mexico, following “intoxication by an undetermined substance”. It turns out the substance may have been carbon monoxide from a gas leak. In John, we lost a dear friend and ally in the freedom and truth movement, someone who’s passion to understand the complexities of our interaction with this virus had drawn him to Geert, and Geert’s work. A very sad loss, a loss of someone who had increasingly become a key support pillar for Geert. So when Geert reached out to me after returning from California for a celebration of John and Abby's lives, asking if we might publish the article through ANH, we were only too happy to help.

Geert Vanden Bossche (left) and John Heathco (right) in Vienna, September 2022
So we too, make this dedication to John and to Abby. Fly free, together, without limits.
In a nutshell
In his article, Geert Vanden Bossche sends a stark warning to those contemplating more C-XX shots later this year, as we proceed towards the northern hemisphere winter. He explains in great detail how and why highly C-XX vaccinated populations will:
- serve to drive ever more infectious and potentially dangerous, immune escape, Omicron-derived variants
- be at greater risk of severe C-XX than less vaccinated or unvaccinated populations, and
- how the risk of other conditions among highly vaccinated populations, including aggressive, early-onset, ‘turbo’ cancers and autoimmune flare-ups, will likely increase significantly compared with those who choose to avoid further C-XX vaccination.
The evidence base pointing in this direction is becoming ever stronger (with many references being made to other literature in Geert’s report). What is more a matter of debate is the mechanisms driving specific interactions, as opposed to the end result. The objective and deterministic world that has delivered so much technology seems incapable of accepting something unless a mechanism is given. Observation, measurement or experience on their own are not enough. We all crave knowing why and how something happens, and we’ll so often deny it’s existence if we’re not given an explanation for how it works.
Knowing what we already know, it is a travesty that such large swathes of the public still have confidence in C-XX vaccines, the vehemence of this position in the public’s mind reflecting the power of the machine driving the agenda.
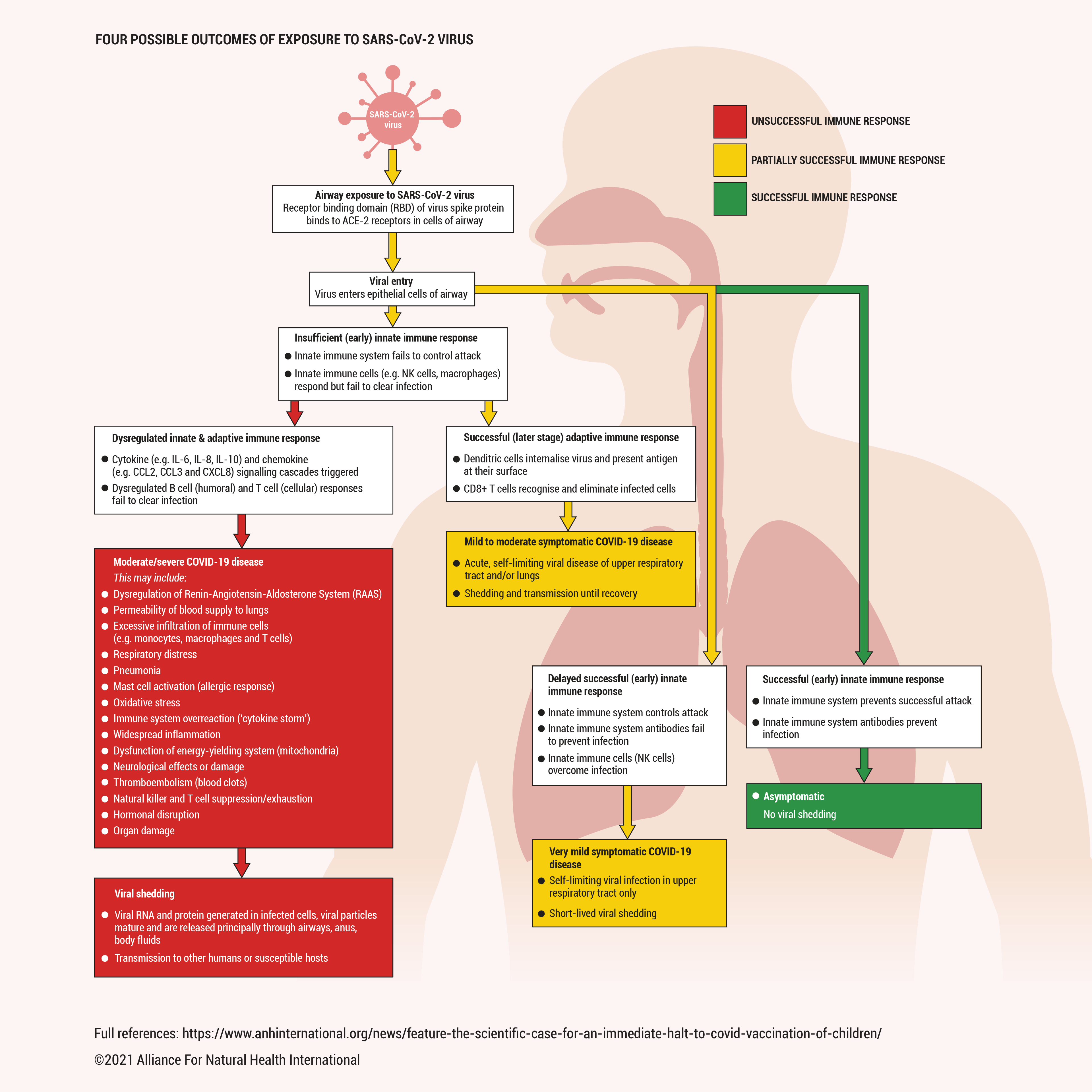
In the simplest terms I can muster, this is what Geert is suggesting is going on, including the elements that are a well-known part of the immune cascade that occurs following infection or vaccination.
What Geert argues is that if you keep vaccinating large cohorts of people while the mutation-prone virus continues to circulate (i.e. during a pandemic), the cascade of events moves in a different direction to that which occurs with natural infection from a virus that enters via the respiratory system.
C-XX vaccination induces a range of immune responses, the target as far as vaccine makers are concerned being the neutralising antibodies made in the B cells of the adaptive immune system that take some weeks to mount an optimal response. For vaccinees, this immune response is triggered by the slightly modified version of the virus’ spike protein that is expressed in cells of the body, but of course, most also encounter the wild virus that infects the upper respiratory tract.
What has been revealed without any doubt over the last couple of years is that these all-important neutralising antibodies don’t work effectively within the context of an immune escape pandemic. That’s been especially the case since the Omicron variant evolved, itself being a response to the extreme immune selection pressure from mass vaccination.
The hope had been that when a vaccinated person becomes infected with the real virus, these neutralising antibodies would bind primarily to the receptor-binding domain (RBD) displayed at the end of the coronaviruses spikes around the surface of the virus. These in turn block the ability of the virus to dock with ACE2 receptors even when the RBDs are in their primed, ‘open’ position, and it is the ACE2 receptors on the epithelial cells of our bodies; these receptors provide the doorways that allow these viruses into our bodies, assuming they haven’t been blocked by the neutralising antibodies.
But, in the case of large parts of the population are vaccinated while being exposed to the virus, these neutralising antibodies do the job imperfectly because their affinity and/or titers (or: concentration in the blood) are still too low when they encounter the virus. This is because, after infection, it takes a few weeks for these antibodies to proliferate and mature in germinal centers and to (get them to) perform at their best.
There’s also another kind of antibody produced by B cells, called non-neutralising antibodies. These are typically elicited in the presence of vaccinal Abs with strongly diminished neutralizing capacity; they are short-lived and do not mature into high-affinity antibodies. As their production is thought to be triggered by a repetitive antigenic pattern displayed on multimeric viral assemblies (so-called viral aggregates) they are called ‘polyreactive’ non-neutralising antibodies (PNNAbs). These antibodies bind to the virus but instead of neutralising the virus, they enhance its entry into susceptible epithelial cells, thereby causing PNNAb-dependent enhancement of viral infectiousness.
One of the features of the early Omicron-derived immune escape variants was that they drove repeated re-stimulation of PNNAbs in vaccinees (due to the strongly diminished neutralizing capacity of vaccine-induced Abs) and history was made when Omicron became the first SARS-CoV-2 variant to cause PNNAb-dependent breakthrough infections in heavily vaccinated populations. This contrasts with the immune escape variants that circulated prior to Omicron. Resemblance of their spike protein to the one used in the vaccines was still good enough to drive ‘original antigenic sin’, that we explained in an article we published on our website in November 2021 (see image from this article above) on which Geert and I collaborated. These variants, therefore, recalled previously vaccine-induced antibodies. However, as the latter became increasingly less effective in neutralizing newly emerging variants, the ‘antigenic sin’ effect only contributed to furthering viral immune escape.
But, sadly, it doesn’t end there. Complications arise because there are multiple classes of antibodies. Many will have heard that the neutralising antibodies belong to a group of proteins called immunoglobulins of which there are multiple classes or isotypes, notably A, D, E, G and M, giving the names IgA, IgD, IgE, IgG, IgM, and so on. These in turn have subclasses, and one that is central to Geert’s concern is one of SARS-CoV-2 spike-specific IgG subclasses called IgG4. Making matters more complicated, the immune system, being as versatile as it is, also has the capacity to engage in immunoglobulin class switching, sometimes also known as isotype switching.
While there’s been a lot of work showing IgG and IgA are elevated for a number of weeks post infection or vaccination, there is now a clear sense that one sub-class of IgG that is normally present at the lowest levels, IgG4, is becoming more prevalent, especially as a result of delayed affinity maturation into a class switched IgG4 isotype in those who are heavily vaccinated without prior infection. This therefore applies to the majority of vulnerable people in heavily vaccinated countries.
This is where things become really interesting – and even more concerning.
Two clear mechanisms appear to operate in parallel.
Firstly, the PNNAb-driven breakthrough infections cause a phenomenon known as steric immune refocusing (SIR) which causes insufficiently neutralising anti-spike antibodies to bind weakly (or: with low affinity) to the ‘immune dominant’ domains of the spike of SARS-CoV-2 (primarily situated within the RBD). As their binding masks the 'immunodominant’ parts of the spike antigen, other spike-associated domains that are subdominant or immune recessive are no longer outcompeted for eliciting their own, broadly neutralizing antibodies. However, as the latter are directed to weakly immunogenic domains (i.e., immune subdominant or immune recessive), titers of these antibodies are low and rapidly decrease, thereby fostering enhanced immune escape.
Secondly, there is the all-important elevation of IgG4 titers. The IgG4 class switch appears to be a last-ditch mechanism by the body to try to deal with the lack of effectiveness of both types of neutralising antibodies, and innate immunity which should have delivered the first salvo of attack but failed to do so because Omicron and its descendants cause vaccine breakthrough infections which expedite production of viral progeny and therefore fail to trigger cell-based innate immune cells (e.g. Natural Killer cells). Ongoing large-scale vaccine breakthrough infections due to more infectious Omicron descendants then place continuous immune selection pressure on circulating viruses that continue to try and work around the body’s defences. The lack of sterilising immunity coupled with the immune selection pressure towards newly emerging immune escape variants means that a cycle is set up in highly vaccinated populations that have no mechanism to dampen out circulating infection. More and new breakthrough variants are created, and the cycle goes on - and on, with no development of true herd immunity.
This loop is something that wouldn’t have occurred if populations had not been massively vaccinated during this pandemic. mRNA vaccines are only expediting immune escape as they promote immune refocusing (refer to Geert’s book, The Inescapable Immune Escape Pandemic, published February 2023). That’s because the innate immune system would have been triggered, therefore trained and have come to the rescue, delivering natural killer cells and other biochemical and cellular weaponry that would have nailed infection much earlier, as it did in children (who have highly effective innate immune systems) during the early days, weeks and months of the pandemic, before the vaccines were introduced.
The process of steric immune refocusing (SIR) combined with delayed IgG class-switching to IgG4 that may in the short-term lessen symptomatic infection appears to also side-line the innate immune system. Not only that, it severely compromises antigen presentation and thereby prevents sustained stimulation of PNNAbs, which likely protect vaccinees from severe disease. While shifting protective adaptive immune responses from long-lived to short-lived, SIR and elevated IgG4 Ab titers are also driving large-scale immune escape which may ultimately turn new, more infectious, immune escape variants into lineages of the virus that are highly virulent in fully vaccinated individuals.

IgG4 has widely been regarded as benign or even beneficial in health and disease, the latter owing to its well described and often helpful response when encountering allergens or parasites. But there is a growing body of research showing that elevated IgG4 titers in the bloodstream, something that tends to be more common in chronic, long-term infections – and now with C-XX mass vaccination – may be detrimental and can be particularly problematic as it compromises antitumour responses and is associated with flare-up of autoimmune diseases. Some of the latest perspectives on this Jeckyll & Hyde nature of IgG4 is laid out in a recent review in Nature Reviews Immunology.
This is exactly the emerging picture we are dealing with; highly aggressive, ‘turbo’ cancers and autoimmune flare-ups among the heavily vaccinated are being reported by exactly the same clutch of doctors and practitioners who first reported success with early treatments against C-XX, including ivermectin. That practitioner group was then silenced and marginalised. The truth, it seemed, was inconvenient.
Are we seeing a repeat of recent history? Are we inching ever closer to a time when authorities will be forcing the masses to line up once again for more shots as symptomatic C-XX disease rises (an uptick is already being noted in some official records), in the blind hope that a failed technology that’s generated the problem might now resolve it?
When will we learn? Or, should we take better note of a quote that is often misattributed to Einstein, “Insanity is doing the same thing over and over again and expecting different results?"
Originally published by Alliance for Natural Health International.








Comments
Post a Comment