Do any treatments reduce the risk of infection after you've been exposed to someone with COVID-19?
There are currently no FDA authorized or approved drugs for post-exposure
prevention of COVID-19 due to the Omicron variant. However, there are several
drugs, including bebtelovimab, Lagevrio (molnupiravir), and Paxlovid
(nirmatrelvir plus ritonavir), that are authorized to treat mild to moderate
COVID-19 if given early to certain patients (one of which is strongly
recommended by the World Health Organization (WHO)), and one drug — remdesivir
(Veklury) — that is approved for use in treating mild, moderate or severe
COVID-19 in some individuals.
The Panel’s recommendations take into account the efficacies of these drugs and the high prevalence of the Omicron VOC. When resources are limited, therapy should be prioritized for patients who are at the highest risk of progressing to severe COVID-19.
The Panel’s current outpatient treatment recommendations are as follows (in order of preference):
In March 2022, the Biden administration launched the Test to Treat initiative. The initiative’s goal was to allow people to be tested for COVID-19 at pharmacies or health centers that have an on-site clinic, like CVS MinuteClinic. If you had a positive test, you’d then receive an antiviral prescription at the pharmacy before leaving the building.
While well-intentioned, there were many roadblocks that made the Test to Treat initiative difficult to roll out. One big barrier was the fact that most pharmacies don’t have clinics in the same building. In late May 2022, there were only about 2,500 Test to Treat locations in the entire U.S. This left many Americans still struggling to get a prescription from their healthcare providers in enough time to benefit from Paxlovid.
In response to this, the FDA updated Paxlovid’s EUA in July 2022. This change allows pharmacists to prescribe Paxlovid directly to people who have tested positive for COVID-19. This means that you might be able to head over to your local pharmacy for the medication without having to make other stops along the way. Keep in mind that not all pharmacies may offer this service.
There is also a monoclonal antibody therapy (EVUSHELD) for pre-exposure
prophylaxis of COVID-19 in certain people. The FDA had previously authorized
three other monoclonal antibody combination therapies — REGEN-COV (casirivimab
plus imdevimab), bamlanivimab plus etesevimab, and sotrovimab — for treatment
of mild to moderate COVID-19 and (for REGEN-COV and bamlanivimab plus
etesevimab) to help prevent infection in people exposed to someone with
COVID-19, but these monoclonal antibody therapies are no longer authorized for
use in any U.S. state.
The COVID-19 Treatment Guidelines Panel’s Statement on Therapies for High-Risk, Nonhospitalized Patients With Mild to Moderate COVID-19 (Last Updated: April 8, 2022)
This statement contains the Panel’s recommendations for treating these
non-hospitalized patients using the currently available therapies.
The Panel’s recommendations take into account the efficacies of these drugs and the high prevalence of the Omicron VOC. When resources are limited, therapy should be prioritized for patients who are at the highest risk of progressing to severe COVID-19.
The Panel’s current outpatient treatment recommendations are as follows (in order of preference):
Preferred Therapies
- Paxlovid (nirmatrelvir 300 mg plus ritonavir 100 mg) orally twice daily for 5 days
- Remdesivir 200 mg IV on Day 1 followed by remdesivir 100 mg IV on Days 2 and 3
Alternative Therapies
For use only when neither of the preferred therapies are available,
feasible to use, or clinically appropriate. Listed in alphabetical
order:
- Bebtelovimab (monoclonal antibody from Eli Lilly)
- Molnupiravir 800 mg orally twice daily for 5 days
- Bebtelovimab is active in vitro against all circulating Omicron subvariants, but there are no clinical efficacy data from placebo-controlled trials that evaluated the use of bebtelovimab in patients who are at high risk of progressing to severe COVID-19. Therefore, bebtelovimab should be used only when the preferred treatment options are not available, feasible to use, or clinically appropriate.
How to Get Paxlovid Without a Medical Doctor
While well-intentioned, there were many roadblocks that made the Test to Treat initiative difficult to roll out. One big barrier was the fact that most pharmacies don’t have clinics in the same building. In late May 2022, there were only about 2,500 Test to Treat locations in the entire U.S. This left many Americans still struggling to get a prescription from their healthcare providers in enough time to benefit from Paxlovid.
In response to this, the FDA updated Paxlovid’s EUA in July 2022. This change allows pharmacists to prescribe Paxlovid directly to people who have tested positive for COVID-19. This means that you might be able to head over to your local pharmacy for the medication without having to make other stops along the way. Keep in mind that not all pharmacies may offer this service.
To get Paxlovid from your pharmacist, you must bring the following documents with you to the pharmacy:
- Your current health records, which must be less than a year old (either electronic or printed records are fine)
- Your most recent liver and kidney function tests, which must be less than a year old
- A complete list of all medications that you take, including any over-the-counter (OTC) medications, vitamins, and supplements
New Paxlovid Dose Pack Authorized by FDA
On April 14, 2022, the U.S. Food and Drug Administration (FDA) revised the
Emergency Use Authorization (EUA) for the COVID-19 oral antiviral
therapeutic Paxlovid to authorize an additional dose pack presentation
with appropriate dosing for patients with moderate renal impairment within
the scope of the EUA. As a result, Paxlovid will soon be available in two
package presentations:
- The standard packaging that is currently in distribution: 300 mg nirmatrelvir;100 mg ritonavir - Each carton contains 30 tablets divided in 5 daily-dose blister cards. Each blister card contains 4 nirmatrelvir tablets (150 mg each) and 2 ritonavir tablets (100 mg each). Nirmatrelvir tablets and ritonavir tablets are supplied in separate blister cavities within the same child-resistant blister card.
- The new packaging option that will be in distribution later this month: 150 mg nirmatrelvir; 100 mg ritonavir - Each carton contains 20 tablets divided in 5 daily-dose blister cards. Each blister card contains 2 nirmatrelvir tablets (150 mg each) and 2 ritonavir tablets (100 mg each). Nirmatrelvir tablets and ritonavir tablets are supplied in separate blister cavities within the same child-resistant blister card.
The updated provider Fact Sheet, Letter of Authorization, and Dear Healthcare Provider Letter are available for reference.
Precaution: PAXLOVID is not recommended (the appropriate
dose has not been determined) in patients with severe renal impairment
(<30 mL/min). (Source)
Paxlovid Doesn’t Work for Healthier Patients, Pfizer Says (Time.com - June 2022)
Pfizer Inc. plans to stop enrollment in a study of its COVID-19 drug in
patients who aren’t at high risk of severe disease after the pill didn’t
help alleviate their symptoms, a major setback for broader use of the
treatment.
The New York-based drugmaker said Tuesday that it would stop adding new participants to a highly anticipated study testing Paxlovid in a broader population of COVID patients who are at low risk of hospitalization and death. The decision comes after the study failed to demonstrate that the drug reduced COVID symptoms among relatively healthy patients and wasn’t able to show a statistically significant reduction in hospitalization and death.
The New York-based drugmaker said Tuesday that it would stop adding new participants to a highly anticipated study testing Paxlovid in a broader population of COVID patients who are at low risk of hospitalization and death. The decision comes after the study failed to demonstrate that the drug reduced COVID symptoms among relatively healthy patients and wasn’t able to show a statistically significant reduction in hospitalization and death.
Paxlovid Rebound
In late May 2022, the CDC
issued a health advisory
about “COVID-19 rebound” after Paxlovid treatment. The CDC described it as “a
recurrence of COVID-19 symptoms or a new positive viral test after having
tested negative.”
At the same time, the CDC wrote, “a brief return of symptoms may be part of the natural history of [coronavirus] infection in some persons, independent of treatment with Paxlovid and regardless of vaccination status.”
The CDC said there is no evidence for more treatment in rebound cases, though people should isolate again for at least 5 days so they won’t pass COVID-19 to others.
People who have a rebound after taking Paxlovid can report their cases to Pfizer’s adverse event reporting page.
At the same time, the CDC wrote, “a brief return of symptoms may be part of the natural history of [coronavirus] infection in some persons, independent of treatment with Paxlovid and regardless of vaccination status.”
The CDC said there is no evidence for more treatment in rebound cases, though people should isolate again for at least 5 days so they won’t pass COVID-19 to others.
People who have a rebound after taking Paxlovid can report their cases to Pfizer’s adverse event reporting page.
FLCCC I-PREVENT Chronic Prevention Protocol
CHRONIC PREVENTION (In order of priority; not all required)
- Ivermectin: 0.2 mg/kg – start treatment with one dose, take second dose 48 hours later, then 1 dose every 7 days (weekly). Those at high risk of contracting COVID-19 can consider dosing twice a week. See Table 1 for help with calculating correct dose. Due to a possible interaction between quercetin and ivermectin, these drugs should be staggered throughout the day. For COVID treatment, ivermectin is best taken with a meal or just following a meal, for greater absorption.
- Zinc: 30-40 mg daily. Zinc supplements come in various forms (e.g., zinc sulfate, zinc citrate and zinc gluconate).
- Melatonin: Begin with 1 mg and increase as tolerated to 6 mg before bedtime (causes drowsiness). Slow- or extended-release formulations preferred.
- Mouthwash: three times a day. Gargle three times a day (do not swallow) with an antiseptic-antimicrobial mouthwash containing chlorhexidine, cetylpyridinium chloride (e.g., Scope™, Act™, Crest™) or povidone-iodine (e.g. Betadine® Antiseptic Sore Throat Gargle™).
- Steam inhalation: once a day. Inhaled steam supplemented with antimicrobial essential oils (e.g., Vicks VapoRub™ inhalations) has been demonstrated to have virucidal activity. Antimicrobial essential oils include lavender, thyme, peppermint, cinnamon, eucalyptus and sage.
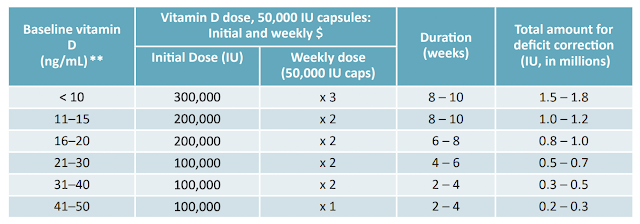
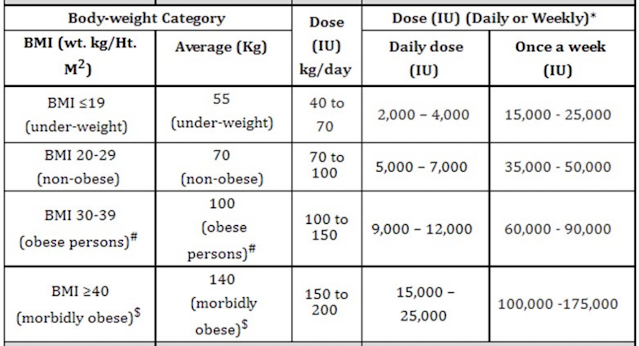
- Vitamin D: dosing varies (see tables below). Vitamin D supplementation is likely a highly effective and cheap intervention to lessen the impact of this disease, particularly in vulnerable populations, (i.e., the elderly, obese, people of color, and those living in northern latitudes). The greatest COVID protection benefit from Vitamin D supplementation will occur in individuals deficient in Vitamin D. Those individuals should take Vitamin D prophylactically on a longer-term basis. When a person with Vitamin D deficiency develops COVID-19, risks increase for developing complications, and Vitamin D supplementation subsequent to infection will have less of a response. Dosing recommendations for Vitamin D supplementation vary widely. The optimal target is over 50 ng/ml; at this level the risk of dying from COVID-19 is extremely reduced. It may take many months or years to achieve optimal levels in patients who are extremely Vitamin D deficient. It is therefore important that the optimal regimen for Vitamin D supplementation for the prophylaxis of COVID-19 is provided promptly, based on baseline Vitamin D levels (see Table 2). If baseline levels are unknown, the needed dose can be calculated from body weight or BMI (see Table 3).
- Curcumin (turmeric): 500 mg twice a day. Curcumin has low solubility in water and is poorly absorbed by the body; consequently, it is traditionally taken with full fat milk and black pepper, which enhance its absorption.
- Nigella sativa (black cumin): 80 mg/kg daily and Honey 1 g/kg daily. Note: thymoquinone (the active ingredient of Nigella sativa) decreases the absorption of cyclosporine and phenytoin. Patients taking these drugs should therefore avoid taking Nigella sativa.
- Vitamin C: 500-1000 mg twice a day.
- Quercetin (or a mixed flavonoid supplement): 250-500 mg daily. Due to a possible interaction between quercetin and ivermectin, these drugs should not be taken simultaneously (i.e., should be staggered at different times of day). As supplemental quercetin has poor solubility and low oral absorption, lecithin-based and nanoparticle formulations are preferred.
- Probiotics. Low levels of Bifidobacterium may predispose a person to COVID-19 and increase disease severity. Likewise, COVID-19 depletes the microbiome of Bifidobacterium, which may then increase the severity and duration of symptoms. Kefir (a fermented milk drink) is high in Bifidobacterium and other probiotics that have demonstrated health benefits. Suggested probiotic supplements include Megasporebiotic (Microbiome labs), TrueBifidoPro (US Enzymes) and yourgutplus+.
Table 1. How to calculate ivermectin dose for chronic prevention

|
| Table 1. How to calculate ivermectin dose for chronic prevention |
Table 2. How to replenish Vitamin D levels based on baseline
levels
|
| Table 2. How to replenish Vitamin D levels based on baseline levels |
Table 3. How to calculate Vitamin D dose when baseline not
available
|
|
Table 3. How to calculate Vitamin D dose when baseline not
available |
FLCCC I-PREVENT Post-Exposure Prevention Protocol
If symptoms develop, treat promptly with
I-CARE protocol. If symptoms do not develop, resume chronic prevention (above) after
one week.
- Ivermectin: 0.4 mg/kg immediately, then repeat second dose in 48 hours. See Table 1 for help calculating dose.
- Hydroxychloroquine (HCQ): 200 mg twice a day for 5 days.
- Zinc: 75-100 mg daily.
- Melatonin: 6 mg daily, at bedtime.
- Mouthwash: three times a day.
- Nasal spray with 1% povidone-iodine: two to three times a day. Sprays such as Immune Mist™, CoFix™ or IoNovo™ administered 2-3 times per day are recommended in post-exposure prophylaxis and in the early phase of COVID-19 infection. Due to low level systemic absorption, povidone-iodine nasal spray should not be used for longer than 5-7 days in pregnant women. IoNovo™ contains iodine in an amount equivalent to the daily dietary requirement and hence is safe to ingest.
- Curcumin (turmeric): 500 mg twice a day for 1 week. Nigella sativa: 80 mg/kg daily for 1 week.
- Vitamin C: 1000 mg twice daily for 1 week.
- Quercetin: 500 mg twice daily for 1 week.
- Probiotics.
- B complex vitamins.








Comments
Post a Comment