Front Line Doctors Long Haul Protocol 2022
Long Haul COVID-19 refers to people who continue to have symptoms weeks after having COVID-19. The symptoms are non-specific. This can be frustrating for both patients and doctors. Long-haul symptoms can occur with other viruses – it is not unique to the SARS-CoV-2 virus.
According to a study of Mayo Clinic patients who had COVID-19, about 75% of the people suffering long COVID symptoms — defined as persistent symptoms even six months after recovery — are women.
How long does long hauler Covid last? LHCS may persist for months after the acute infection and almost half of patients report reduced quality of life. Patients may suffer prolonged neuropsychological symptoms, including multiple domains of cognition. (Ref, Ref)
Another study published in The Lancet suggests that many patients previously hospitalized with Covid-19 have experienced lingering symptoms for months. And for nearly half of them, at least one symptom has persisted past the one-year mark.

Researchers are learning new details about the long-term effects of COVID-19. A study shows COVID-19 "long haulers" have a significantly higher chance of dying months after their infection.
According to the paper in Nature, COVID survivors have a 59 percent higher risk of death within six months of contracting the virus.
Symptoms of Long Haulers Syndrome
Clinical signs and symptoms can be grouped in the following clusters. The reason for this grouping is to allow organ specific targeted therapy/individualized therapy.
1. Respiratory: shortness of breath, congestion, persistent cough, etc.
2. Neurological/psychiatric: brain fog, malaise, tiredness, headaches, migraines, depression, inability to focus/concentrate, altered cognition, insomnia, vertigo, panic attacks, tinnitus, anosmia, phantom smells, etc.
3. Musculoskeletal: myalgias, fatigue, weakness, joint pains, inability to exercise, post-exertional malaise, inability to perform normal activities of daily life (ADL’s).
4. Cardiovascular: Palpitations, arrhythmias, Raynaud like syndrome, hypotension, and tachycardia on exertion.
5. Autonomic: Postural tachycardia syndrome (POTs), abnormal sweating.
6. GIT disturbance: Anorexia, diarrhea, bloating, vomiting, nausea, etc.
7. Dermatologic: Itching, rashes, dermatographia
8. Mucus membranes: Running nose, sneezing, Burning and itchy eyes.
9. Auditory: tinnitus, hearing loss and vertigo. (International Journal of Audiology, Nature)
FLCCC I-Recover Protocol
Given the lack of clinical trials of long-haul COVID-19 syndrome, these recommendations are based on the abnormal changes within the body associated with the COVID-19 disease and post viral illnesses along with the collective experience of FLCCC members.
This protocol has also been used to treat post-vaccine inflammatory syndromes with similar success. As with all FLCCC Alliance protocols, the components, doses, and durations will evolve as more clinical data accumulates.
The I-Recover protocol has been updated and below is their latest version (version 2: Jan 20, 2022).

First-line treatments based on the FLCCC I-Recover Protocol.
- Ivermectin: 0.2mg/kg body weight. Once daily for 1 week. Discontinue after 2 - 4 weeks if all symptoms have resolved. A repeat course is recommended in those who respond poorly or relapse once the treatment is stopped. The anti-inflammatory properties of ivermectin may mediate this benefit. (Find a Doctor)
- Prednisone: 10–15mg daily for 3 weeks. Taper to 10mg for three days, then 5mg for three days and then stop.
- Low dose naltrexone (LDN): Begin with 1 mg daily and increase to 4.5mg as required. May take 2–3 months for full effect.
- Omega-3 fatty acids: Vascepa, Lovaza or DHA/EPA 4g per day. Omega-3 fatty acids play an important role in the resolution of inflammation by inducing resolvin production. [Ref, Ref]
- If symptoms do not improve after 1–2 weeks continue steroids, omega-3 fatty acids and Naltrexone and add second line medications.
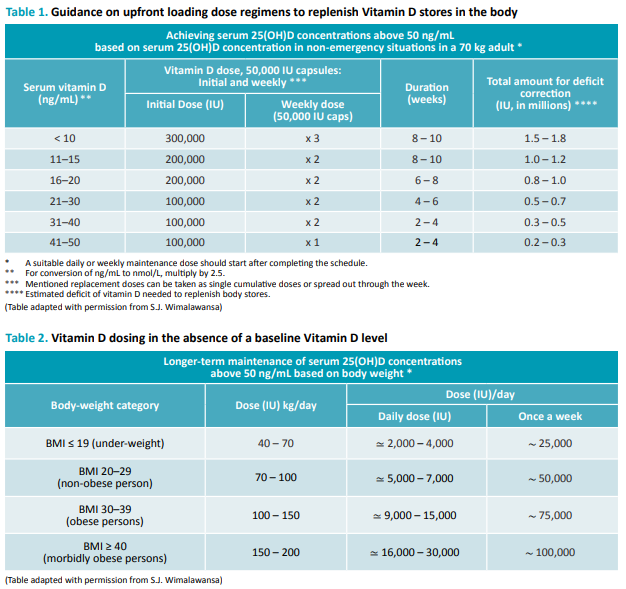
- Vitamin D: The majority of those with post-COVID-19 syndrome continue to have hypovitaminosis D. See tables 1 or 2 for vitamin D supplementation.
2nd Line Therapies
- Fluvoxamine (low dose): 25mg once daily. Stop if the symptoms increase. Caution with the use of other antidepressants and psychiatric drugs. Taper and discontinue once symptoms improve.
- Atorvastatin: 20–40mg once daily. Caution in patients with Postural Orthostatic Tachycardia Syndrome (POTS); may exacerbate symptoms.
3rd Line Therapy
- Maraviroc: 300mg PO twice a day If 6–8 weeks have elapsed and significant symptoms persist, consider either getting an InCellDx test to assess long hauler index profile prior to initiating or can consider initiating empirically. Note maraviroc can be expensive and it has risk for significant side effects and drug interactions.
4. Optional adjunctive therapies (in order of priority)
- Curcumin: has anti-inflammatory and immunomodulating properties and has been demonstrated to repolarize macrophages.
- Nigella Sativa: which like curcumin has anti-inflammatory and immunomodulating properties.
- Vitamin C: 500mg BID (vitamin C inhibits histamine and repolarizes monocytes). [Ref]
- Melatonin: 2–8mg at night (slow release/extended release) with attention to sleep hygiene. Increase dose from 1mg as tolerated (may cause severe nightmares at high dosages).
- Kefir, probiotic yogurt and/or Bifidobacterium Probiotics (e.g., Daily Body Restore) together with Prebiotics (e.g. XOS Prebiotic, Bio Nutrition Pre-Biotic) to normalize the microbiome. Prolonged dysbiosis has been reported following COVID-19 infection.
- Behavioral modification, mindfulness therapy and psychological support may help improve survivors’ overall well-being and mental health.
- Luteolin 100–200mg day or Quercetin 250mg day (or mixed flavonoids). Luteolin and quercetin have broad spectrum anti-inflammatory properties. These natural flavonoids inhibit mast cells, and have been demonstrated to reduce neuroinflammation.
- H1 receptor blockers (for mast cell activation syndrome): Loratadine 10mg daily, or Cetirizine 5–10mg daily, or Fexofenadine 180mg — daily.
- H2 receptor blockers (for mast cell activation syndrome): Famotidine 20–40mg, or Nizatidine 150mg — twice daily as tolerated.
- Montelukast: 10mg/day (for mast cell activation syndrome). Caution as may cause depression in some patients.
- Anti-androgen therapy: Spironolactone 50–100mg twice a day, and Dutasteride 1mg daily.
Mast cell stabilisers: rupadatadine, quercetin or luteolin.








Comments
Post a Comment