Dr Chris Centeno: Omicron Update and More Zombie Apocolypse Misinformation
I’m still on a holiday blogging schedule, but a patient just sent a whacky blog on Omicron so I thought it was time to respond. So here’s an update on all things Omicron. Let’s dig in.
Omicron Hospitalization Update
Early on in this pandemic, the epidemiologists had a message that was quickly drowned out by the media. That message was simple. There was no way to avoid the total number of deaths that would happen, as we didn’t have treatments and we didn’t have vaccinations back then. The only thing shutdowns would do is to “flatten the curve”. Hence, it was all about protecting the hospital systems. Meaning moving hospitalizations that might happen in March of 2020 into April or May.
Here at the end of December of 2021, the only metric we should be paying attention to is hospitalizations. Why? We have a highly infectious variant that will likely infect most people. Each time it does that and someone recovers, they have immunity. If that person was vaccinated, then based on what’s being observed, there is super immunity (3). However, we have a fixed number of hospital and ICU beds.
So how will Omicron impact hospital systems? A preprint publication out of South Africa was just published online showing that Omicron causes 80% fewer hospitalizations (2). In addition, of those hospitalized, there was about a 2/3rds less chance of having severe COVID-19. Given that all of this information fits with what the physician who discovered this variant reported early on, this is great news. Basically, the risk of severe disease is about 6% of the Delta variant. Or said another way, it’s 94% less likely. Given those numbers, we’re now likely back down to the virulence of influenza or close to it.
The Placebo Effect
This early South Africa data will be the most accurate we can get. Why? Most of it was collected when people didn’t know much about what was happening with Omicron. Once the media got a hold of this story and whipped everyone into a frenzy, things were bound to change. Meaning that we have all been conditioned to believe that if we got any cold-like symptoms, we could have a potentially fatal disease. Hence, any reasonable person post-pandemic would err on the side of caution and go to the hospital in a situation pre-pandemic that would have never caused a hospital or Emergency Room visit. Hence, we can expect hospital system strain for the next 1-2 months as Omicron becomes the most dominant strain and otherwise well patients with mild Omicron rush to hospitals.
New Omicron Study Shows that It’s Likely a Blessing in Disguise
The Africa Health Research Institute just published a study on its website that shows that not only did Omicron out-compete the Delta variant, but that because it increases antibodies making people able to fight Delta, that this variant likely signals the end of the pandemic and beginning of the endemic (11). The graph below shows that while Omocron neutralizing antibodies went up 14X after infection (as expected), the ability to fight the Delta strain also went up on average 4X:
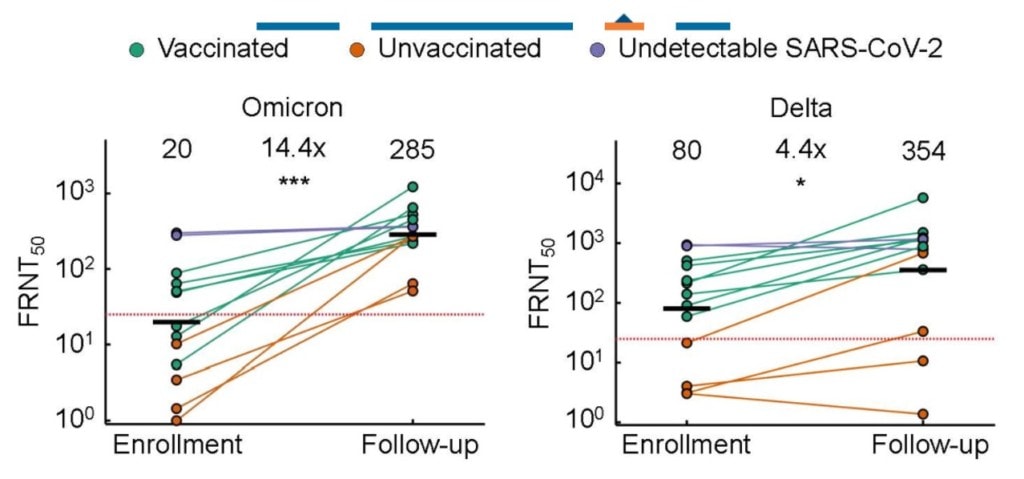
Only 1 of the 15 patients tested didn’t have this enhanced ability to fight Delta. Hence, the researchers believed that Omicron will likely move us from a pandemic to COVID being just another endemic disease that exists out there that we need to be prepared to fight in select patients.
The CDC Reduces Quarantine Requirements
Omicron runs through the body fast. After 4-5 days, people are no longer infectious. Hence the CDC just reduced quarantine from 10 days to 5 days (1). That’s a super hopeful sign that our CDC is following the science and readily adapting to what we know about Omicron. So kudos to the CDC!
Omicron as a Harbinger of the Zombie Apocolypse
A young writer, Omar Haque, with a 4-year neuroscience degree and whose science education on this topic, therefore, is limited to a single college biology class (the same one anyone with a STEM degree took) has written a blog post entitled, “Why the Pandemic Won’t End. We’re Trapped in a Covid Doom Loop”. What other science qualifications does Omar have? He has an MBA and is an expert on consumer branding, so absolutely zero.
The basic premise of this post that was written to garner clicks (as any good marketing professional would create) is:
- Viruses can mutate to become more severe
- Coronaviruses are great at mixing in new DNA
- Omicron is more infectious
- The pandemic will never end
- Hence, we need to shut the whole world down for about a month and vaccinate every living soul on the planet
- If we don’t do this, then we risk another worldwide plague
Why is all of this fear-mongering without much substance?
Viruses Mutate and Evolution Does the Selecting
Viruses do what they do, which is to make copies of themselves. All they “know” is that they want to continue to make more copies. Evolution then selects out a virus that can infect as many people as possible in as short a time as possible.
In this game of viral spread, we have a few evolutionary pressures to consider. Killing the host quickly reduces the number of people you can infect. In fact, in today’s world, since sick people end up in the hospital, making someone sick enough to be hospitalized is also a problem for viral spread. Why? Once that person is admitted into a system designed to reduce the spread of communicable disease (the modern hospital), the game is up. The likelihood of the virus spreading to other patients goes way down. In addition, on the other end of that equation is the power of the human immune system. The longer you live inside a person, the more likely it is that you will be killed off by antibodies or T-cells.
Hence, viruses tend to be selected to become milder and quicker (in and out of the body in less time). Not because anything changes with the virus or because it has certain wishes, but because that’s the way evolution works. Take for example the MERS virus. It killed hosts quickly and only became infectious when people were admitted to the ICU, so few people died from MERS and it died out quickly. The original COVID strain and Delta were better from an evolutionary standpoint in that they could infect people and it would be at least a week or more before a tiny fraction of those people got admitted to the hospital. Now evolution has selected Omicron because it causes mild disease in about 20X more people, so it can maximize its spread. It’s also more transmissible. So it quickly becomes the dominant strain. What would happen if it suddenly mutated to become more deadly? Its ability to spread would go way down.
The Pandemic Will Never End
Just like cold coronaviruses spike in frequency every winter, this one will likely do the same, so this assertion has some truth. However, that should be weighed against COVID “super immunity”. This is what happens when a vaccinated person becomes infected. There is very high immunity that crosses over to other coronaviruses, even of the common cold variety (3). While some recent research shows that this too wanes with time, it’s still higher than natural immunity (4). So will our existing vaccination strategy combined with almost certain infections with Omicron be enough to eradicate Omicron and other COVID viruses? Too early to tell. If not, we will all get used to more vaccinations and living with COVID.
Shutting Down AGAIN?
We are now beginning to understand the effects of shutdowns and other mitigation measures on society. For example, cancer screenings and diagnoses plummeted (5,6). This will of course lead to many more otherwise preventable cancer deaths. There were also measurable impacts on mental health with spikes in depression, substance abuse, anxiety, etc (7). Suicide rates among black residents in one state where they were tracked exploded 94% (8). While the total health impacts of the shutdowns of 2020 will take years to figure out, we do know that shutting down society is not a zero-sum game. You gain lives on one side of the ledger and lose them on the other. Shutting down for a low virulence virus variant like Omicron, therefore, makes even less sense from a public health standpoint.
Related: Britain got it wrong on Covid: long lockdown did more harm than good, says scientist (The Guardian)Plague 2.0?
Haque (the marketing guru) predicts that we are risking yet another Plague if we don’t follow his sage advice. He refers to the middle ages Bubonic Plague which had a very high mortality rate, killing between 20-40% of the people in Europe. However, that won’t happen again. Why?
The bug that caused the Bubonic Plague was a bacterium called Yersinia Pestis that could be killed easily by modern antibiotics. Meaning the “black death” all happened before there was a scientific theory and modern medicine. In today’s world, in just a year, we’ve developed many different effective treatments for COVID. These include vaccines as prevention, monoclonal antibodies, and now new oral antiviral pills that have just received US FDA EUA (9,10 ). So even if we saw a more virulent strain happen to spread, given the mRNA vaccine technology developed and used in this pandemic, a new vaccine could be cooked up in months. Hence, the idea that we could have another Plague where one quarter to half of the world population dies is ridiculous. However, that’s what you get when you put a marketing guy with a single college biology class under his belt in charge of public health policy.
The Real Problem?
So if it’s not credible that we’re careening toward another worldwide Plague event, what are the risks here with Omicron? Our real risk is repeating all of the mistakes of the past 18-months. What we should have done from the outset with COVID was:
- Protect the elderly and at-risk people
- Make public health decisions to avoid medical system overload
- Get everyone vaccinated as quickly as possible
- Continue to develop effective treatments for COVID
After returning from a local Whole Foods and seeing again the pandemic panic in the eyes of many shoppers, we are again failing here. A mild variant that is highly infectious in a world with next-level vaccination technology and advanced medicine should be a good thing, not a cause for abject panic. So our real problem is not the virus that evolution selected, but our human knee-jerk responses to that virus.
The upshot? Will we get it right for the Omicron wave? On the one hand, I’m optimistic based on the CDC’s recent change in Quarantine requirements. However, the media as usual is getting this one more wrong than right. Our stories should be focused on one thing. How are our hospitals holding up? More and more reporting on case numbers or a silly blog post by a marketing guy are again causing more harm than good.
_______________________________________________________________
References:
(1) CDC. CDC Updates and Shortens Recommended Isolation and Quarantine Period for General Population. https://www.cdc.gov/media/releases/2021/s1227-isolation-quarantine-guidance.html
(2) Wolter N, et al. Early assessment of the clinical severity of the SARS-CoV-2 Omicron variant in South Africa. medRxiv 2021.12.21.21268116; doi: https://doi.org/10.1101/2021.12.21.21268116
(3) Wang Z, Muecksch F, Schaefer-Babajew D, et al. Naturally enhanced neutralizing breadth against SARS-CoV-2 one year after infection. Nature. 2021;595(7867):426-431. doi:10.1038/s41586-021-03696-9
(4) Goldberg Y, et al. Protection and waning of natural and hybrid COVID-19 immunity. medRxiv 2021.12.04.21267114; doi: https://doi.org/10.1101/2021.12.04.21267114
(5) Asai Y, et al. Impact of the COVID-19 pandemic on skin cancer diagnosis: A population-based study. Published: March 31, 2021
https://doi.org/10.1371/journal.pone.0248492
(6) Gurney JK, Millar E, Dunn A, Pirie R, Mako M, Manderson J, Hardie C, Jackson CGCA, North R, Ruka M, Scott N, Sarfati D. The impact of the COVID-19 pandemic on cancer diagnosis and service access in New Zealand-a country pursuing COVID-19 elimination. Lancet Reg Health West Pac. 2021 May;10:100127. doi: 10.1016/j.lanwpc.2021.100127. Epub 2021 Mar 22. PMID: 33778794; PMCID: PMC7983868.
(7) KFF. The Implications of COVID-19 for Mental Health and Substance Use https://www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use/
(8) Hopkins Medicine. Suicides Rise in Black Population During COVID-19 Pandemic. https://www.hopkinsmedicine.org/news/articles/suicides-rise-in-black-population-during-covid-19-pandemic
(9) NIH. COVID-19 treatment Guidelines. https://www.covid19treatmentguidelines.nih.gov/therapies/anti-sars-cov-2-antibody-products/anti-sars-cov-2-monoclonal-antibodies/
(10) USFDA. Coronavirus (COVID-19) Update: FDA Authorizes Additional Oral Antiviral for Treatment of COVID-19 in Certain Adults. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-additional-oral-antiviral-treatment-covid-19-certain
(11) Africa Health Research Institute. Omicron infection enhances neutralizing immunity against Delta. https://www.ahri.org/omicron-infection-enhances-neutralising-immunity-against-delta/
Original Article: https://regenexx.com/blog/omicron-update-and-more-zombie-apocolypse-misinformation/







.png)
Comments
Post a Comment