BA.2.86 Variant (Pirola): COVID Variant Spreading in US, but Risk Is Low According to Experts

Current Research Suggests Low Risk of Disease
Pirola is derived from BA.2, an earlier Omicron variant.Other variants derived from BA.2 include XBB.1.5 which became the dominant strain in early 2023.
The current dominant variant is H.V.1, and it is derived from the variant EG.5, unofficially known as Eris, a previously dominant variant in the United States.
“At this time, BA.2.86 does not appear to be driving increases in infections or hospitalizations in the United States,” the CDC wrote.
Research outside of the United States similarly suggests that Pirola should not be more severe than current variants.
Compared to Eris, Pirola has a significantly lower growth efficiency, meaning that it is less capable of replicating itself in the host, the authors wrote.
Prior Infections Gives Immunity Against the New Variant
Compared to BA.2, its ancestral subvariant, Pirola has more than 30 mutations in its spike protein. The virus uses the spike protein to infect human cells.The substantial number of mutations initially raised concerns among virologists, who feared this variant might partially evade earlier immunity from previous exposure, whether from natural infection or prior vaccination.
However, evidence is still lacking to predict if there will be more immune evasions as well as the severity of future Pirola cases.
Mr. Cao’s own research in mice who have been vaccinated or infected with XBB vaccines showed that the antibodies generated “cannot well recognize and neutralize BA.2.86,” he wrote in a thread posted on the social media platform, X.
However, Pirola had a low cell infectivity, which can affect the variant's transmission, he added.
In discussion of Mr. Cao’s findings, Mr. Hanage agreed that immune evasion is not a definite indication of more severe infection and transmission.
The most recent research on Pirola's immune evasion abilities comes from a series of reports conducted by researchers at Columbia University.
These antibodies conferred robust neutralizing activity against Pirola. The authors also noted that Pirola's ability to evade immunity was no better than that of XBB1.5 and EG.5.
HV.1: The Current Dominant Variant
The current dominant subvariant is HV.1, a new variant derived from Eris.Eris is currently the most dominant globally and HV.1 succeeded Eris as the dominating variant in the U.S. on Oct. 28, 2023.
Like Pirola, the WHO has classified HV.1 as a variant with low public health risk. The variant accounted for about 31.5 percent of all cases in the United States as of Nov. 25.
Is HV.1 More Dangerous Than Other COVID Variants?
The COVID-19 variants that gain dominance over others typically do so because they have evolved to become more transmissible.
“My general sense is that the Omicron progeny—the children, grandchildren, and great-grandchildren of Omicron—are, in general, pretty darn transmissible,” said William Schaffner, MD, a professor of infectious diseases at the Vanderbilt University School of Medicine.
However, he added, “they’re not severe. The reassuring information still comes from the immunologists telling us that so far, the vaccine that was created will continue to provide substantial protection against severe disease.”
HV.1 evolved from EG.5 variant, which is a member of the XBB. The updated vaccine is expected to protect against serious illness from HV.1 and other circulating strains, according to Kate Grusich, a public affairs specialist at the CDC. COVID-19 cases also haven’t become notably more severe since the variant’s emergence.Prevent illness in the first place
While we’re at it, let’s talk about getting your immune system into shape, and other evasive actions you can take to make sure you’re strong, healthy, and ready to fight off any virus coming your way this fall.
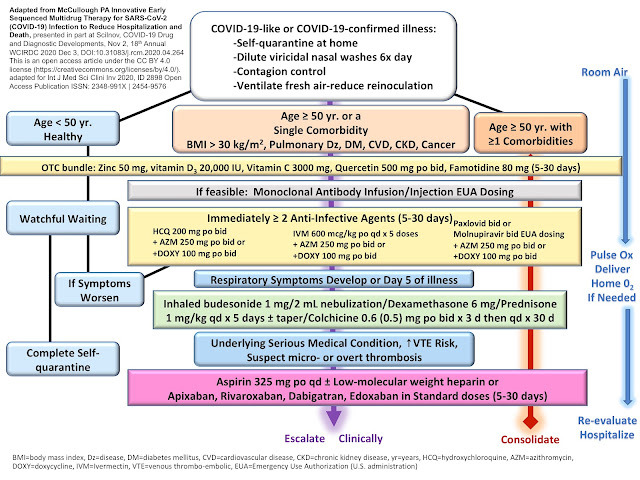
Many people have asked whether they should start up a prophylactic treatment of ivermectin again. On that front, our advice has not really changed: if you have significant comorbidities, lack natural immunity, or have a suppressed immune system you may want to try a twice-weekly dose of ivermectin at 0.2 mg/kg. Likewise, consider it if you are currently suffering from long COVID or post-vaccine syndrome and are not currently being treated with ivermectin. If you have an upcoming situation where you may have high possible exposure — such as travel, weddings, or conferences — taking daily ivermectin starting two days before departure and either daily or every other day during the period of high exposure is a reasonable approach.
Remember to immediately initiate daily ivermectin at treatment doses (0.4 mg/kg) at the first signs of any kind of viral syndrome. It bears repeating: Early treatment is essential!






Comments
Post a Comment