The One-Two Punch Against Spike Proteins: Nattokinase and Ivermectin - Colleen Huber
The One-Two Punch Against Spike Proteins: Nattokinase and Ivermectin
Those who had the mRNA COVID vaccines may be programmed to produce spike proteins for a period of time, for which nobody is yet certain of the duration. In my last Substack essay, I argued that ivermectin and nattokinase are the two most helpful substances I have known to degrade spike proteins and to help COVID-vaccinated people feel better.
Nattokinase is a proteolytic enzyme, so its effect on spike proteins is degradative, chewing up the most problematic S1 and S2 edges, so to speak, to sort of de-fang that molecule. Ivermectin, on the other hand, interferes with the spikes’ docking onto and entry into the cell. So the one-two punch is that nattokinase interferes with spike structure, while ivermectin interferes with spike transport and function.
Purists might prefer to avoid all pharmaceuticals, even ivermectin, even given its squeaky-clean safety history. However, the spike proteins are so dangerous and destructive that my family and I have taken ivermectin at least dozens of times, especially in 2021, after exposure to recently vaccinated individuals, while avoiding all other drugs.
Vitamin C is essential for heart health following an event involving myocarditis risk to replenish collagen, in its supporting role of the remaining cardiomyocytes. There are five types of collagen, each used differently. Collagen in the heart is more Type 1 and Type 3 than any other. Vitamin C is essential for collagen production. I write about that here. The heart uses a lot of vitamin C when it is stressed; 24 hours after bypass surgery, vitamin C plummets by 70 percent. [1] However, after surgery or any assault on the heart, vitamin C is most urgently needed for wound repair. It builds collagen, which is that “bricks and mortar” function I mentioned in my last article.
A Synergy of Nutrients in the Mitochondria
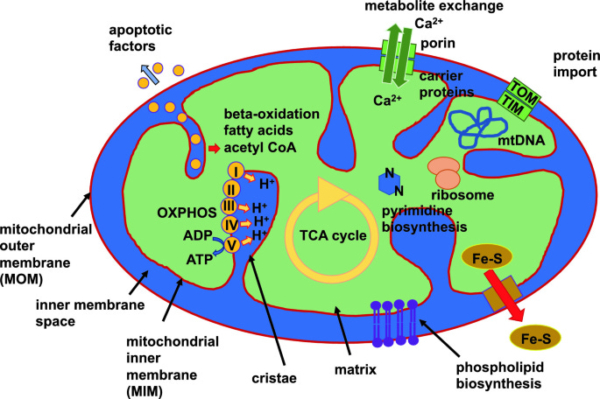
The mitochondria are the sub-cellular units of energy production in the body. They are often portrayed as oval structures in each cell, with busily coordinating, assembly line-type chemical reactions. Here is a very simplified diagram of that activity.
Other Vitamins for Heart Health
Vitamin B5 is pantothenic acid or pantethine. When the heart suffers ischemia, stored pantethine gets used up. Pantethine levels in the blood are inversely related to cardiovascular disease. [2] As part of the transport enzyme CoA, vitamin B5 is known to transport fatty acids in the mitochondria and cell cytoplasm. It is essential to mitochondrial function, which pretty much keeps our engines running. Notice acetyl-CoA near the top of the above diagram. Vitamin B5 is a fundamental component of that, helping to bring digested food molecules into the mitochondria.
Vitamins B2 and B3, or riboflavin and niacin, respectively, help usher metabolism. Where you see NADH and FMNH2 in the upper left of the above diagram, those are derived from niacin and riboflavin, respectively. You see each on a pathway, in cooperative choreography with the other nutrient molecules, each playing its graceful role in optimal metabolic function.
Not Quite a Vitamin: CoQ-10
While in the mitochondria, another nutrient that is not quite considered a vitamin but essential for mitochondrial function is ubiquinone, or CoQ-10. Moving down from NADH and FMNH2 in the upper left of the above diagram, you arrive at UQ (ubiquinone) and UQH2 near the center, well into the electron transport chain, an essential part of energy production. The heart loves CoQ-10, as it seems to impart more resilience. It was found to increase treadmill exercise tolerance. [3] The vicious cycle is that heart disease depletes CoQ-10, [4] while the heart needs CoQ-10 to repair heart disease. [5] Three out of four patients with heart disease have low CoQ-10. [6] CoQ-10 is often supplemented between 100 and 300 or more milligrams per day.
If you are crazy enough to take a statin drug (yes, crazy or very badly misinformed), then you might as well kiss your heart goodbye. Statins deplete CoQ-10 and are one of the most foolish of commonly used drugs that you can put in your body. Whoever first conned people into fearing their own cholesterol may as well have been selling insurance policies against the sky falling on their heads. Please pardon my brutal frankness; it’s only that loads of people, mostly American seniors, are letting themselves get slowly killed by these drugs.
Amino Acids for the Heart
Carnitine is one of the most appreciated amino acids for the heart. In normal health, the heart stores more carnitine than it needs or uses on a daily basis. Then, in case of angina or myocardial infarction (heart attack), those stores of carnitine become used up; if not replenished, angina recurs. Survival after myocardial infarction was significantly improved when patients were given intravenous L-carnitine. [7] Acute myocardial infarction patients had significantly lower troponin labs (a marker of heart injury after heart attack) when they had been given intravenous carnitine than placebo. [8] A dose of 900 milligrams per day has been shown to improve angina and heart disease, and reduce the size of infarcts, [9] and facilitate mitochondrial function and more efficient use of oxygen. [10]
In my last article, I mentioned lysine and proline as synergistic with vitamin C in the building of new collagen. Both of these amino acids contribute to the structural components of collagen molecules.

Minerals and Electrolytes
Magnesium is considered one of the most common nutritional deficiencies in the United States, as monoculture farming practices deplete our soils of this and other minerals. Yet it is so important to heart health that there is a high correlation between men dying from sudden heart attacks and their having much lower heart stores of magnesium. Of men with chest pain, only about one-quarter died who were treated with magnesium compared to the untreated control group. When acute myocardial infarction patients are supplemented during the first hour after their heart attack with intravenous magnesium, short- and long-term complications and death are greatly reduced. [11] Lack of magnesium produces spasms in the heart, vasospasms, and arrhythmias. [12] Vasospasms are characteristic of angina.
In the case of a heart attack or smaller ischemia (when blood flow to a portion of the heart is choked off by a clot), magnesium is the nutrient to look to first for its vasodilation effect. That is, a clot has choked off essential blood flow (carrying most urgently oxygen, and then nutrients). So the tissue is starved for too long—even a minute is too long. Magnesium’s solution to this problem is vasodilation, which is the widening of blood vessels, which enables collateral flow through more or less parallel vessels, helping to get oxygen to the starved tissue by backdoor sort of routes. This effect has been shown to reduce the size of the damaged area, at least in animal experiments. [13]
The spike proteins threw a new sort of monkey wrench into the heart. Instead of old-fashioned big clots, now there is more microclotting, caused by the spikes jutting into what should be smooth flowing blood through the vessels. These jutting spike protein shards create turbulence and eddies, which give rise to microscopic clots, and essentially more viscous blood. I talked about the fluid dynamics of that here, and how it creates myocarditis risk. However, to some extent, the problem existed even before the COVID era. Even half a century ago, in 53 percent of acute infarction cases, no occlusive thrombus in the artery supplying the infarcted area was found. [14]
Magnesium can help with damaged endothelium and microclotting also. The COVID vaccines’ worst injury generally is to the endothelium. This is the lining of the blood vessels. Magnesium heals and improves the tone of the blood vessel walls, [15] and protects against oxidative endothelial injury. [16]
As for the type of magnesium, magnesium taurate or magnesium glycinate, or magnesium bis-glycinate seem to be better utilized by the neurological, cardiovascular, and musculoskeletal systems than other forms. Some of the other commercially available magnesium supplements are less likely to leave the GI tract, and they can make stools loose. Dosing is best figured out together with a health care provider, who will take into account your heart history, blood pressure, activity level, elimination, tendency to headaches or not, and how much you sweat during exercise, all of which should impact magnesium dosing. Daily dosing is often in the 100 to a few hundred milligrams.
And Now for Something Controversial…
I like salt. Not just because I like the taste, which I do, but also because my exercise is intense and frequent, so I lose salt in sweat, and I need to replace it.
Sodium is often vilified by doctors who have seemingly forgotten some of the biochemistry and physiology lessons they learned in medical school. We may assume such forgetting occurs because sugar has a lobby and salt does not, so salt gets blamed for the problems caused by sugar.
We could not live even another few seconds without sodium; it is impossible to be without it because the sodium-potassium pump drives nearly every process in every organ in the body. This is an exchange of sodium and potassium across the cell membranes everywhere in the body. Sedentary people have been advised to take ½ to 1 teaspoon of clean salt per day. (Watch out for microplastics in sea salt; thanks, billions of discarded disposable masks on beaches and waterways!) But I like that just to start, as active people need even more than that. Also, for potassium, 3,500 to 4,700 milligrams a day is an oft-cited rule of thumb. Potassium is plentiful in whole, natural foods but is especially abundant in avocados and potatoes.
Each of the above substances should be discussed with your local health care provider regarding safety considerations, appropriateness for your health goals, and dosing.
Reposted from Colleen Huber’s Substack
◇ References
[1] Shiraz Univ Med Sci. The effect of high-dose vitamin C on biochemical markers of myocardial injury in coronary artery bypass surgery. Sep 2019. Brazilian J Cardiovasc Surg. https://www.scielo.br/j/rbccv/a/mQWJnpm4L7PjnnNXgw3pgJM/?lang=en
[2] P Sun, H Weng, et al. Association between plasma vitamin B5 and coronary heart disease: Results from a case-control study. Oct 13 2022. Front. Cardiovasc Med. https://www.frontiersin.org/articles/10.3389/fcvm.2022.906232/full
[3] T Kamikawa, A Kobayashi, et al. Effects of coenzyme Q-10 on exercise tolerance in chronic stable angina pectoris. Aug 1985. Am J Cardiol. https://www.sciencedirect.com/science/article/abs/pii/0002914985908434
[4] V Zozina, S Covantev, et al. Coenzyme Q10 in cardiovascular and metabolic diseases: Current state of the problem. Aug 2018. Curr Cardiol Rev. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6131403/
[5] A Kumar, H Kaur. Role of coenzyme Q10 (CoQ10) I cardiac disease, hypertension and Meniere-like syndrome. Dec 2009. Pharmacol Ther. https://pubmed.ncbi.nlm.nih.gov/19638284/
[6] V Zozina, et al. Ibid. Coenzyme Q10 in COPD: An Unexplored Opportunity? – PubMed (nih.gov)
[7] G Tarantini, D Scrutinio, et al. Metabolic treatment with L-carnitine in acute anterior ST segment elevation myocardial infarction: A randomized controlled trial. May 9 2006. Cardiology. https://pubmed.ncbi.nlm.nih.gov/16685128/
[8] Y Xue, L Wang, et al. L-carnitine as an adjunct therapy to percutaneous coronary intervention for non-ST elevation myocardial infarction. Oct 23 2007. Cardiovasc Drugs & Ther. https://link.springer.com/article/10.1007/s10557-007-6056-9
[9] J DiNicolantonio, A Niazi, et al. L-Carnitine for the treatment of acute myocardial infarction. Mar 2014. Rev Cardiovasc Med. https://www.imrpress.com/journal/RCM/15/1/10.3909/ricm0710
[10] M Mollica, S Iossa, et al. Acetyl-L-carnitine treatment stimulates oxygen consumption and biosynthetic function in perfused liver of young and old rats. Mar 2001. Cell Mol Life Sci. https://pubmed.ncbi.nlm.nih.gov/11315193/
[11] M Schechter, H Hod, et al. Magnesium therapy in acute myocardial infarction when patients are not candidates for thrombolytic therapy. Feb 1995. Am J Cardiology. https://www.ajconline.org/article/S0002-9149(99)80546-3/pdf
[12] W Vierling, D Liebscher, et al. [Magnesium deficiency and therapy in cardiac arrhythmias: recommendations of the German Society for Magnesium Research]. [Article in German]. May 2013. Dtsch Med Wochenschr https://pubmed.ncbi.nlm.nih.gov/23700303/
[13] C Chang, J Varghese, et al. Magnesium deficiency and myocardial infarct size in the dog. Feb 1985. J Am Coll Cardiology. https://www.sciencedirect.com/science/article/pii/S0735109785800486?via%3Dihub
[14] G Baroldi. Acute coronary occlusion as a cause of myocardial infarct and sudden coronary heart death. Dec 1965. Am J Cardiology. https://www.ajconline.org/article/0002-9149(65)90704-6/pdf
[15] M Schechter, M Sharir, et al. Oral magnesium therapy improves endothelial function in patient with coronary artery disease. Nov 7 2000. Circulation. https://www.ahajournals.org/doi/10.1161/01.CIR.102.19.2353
[16] P Pearson, P Evora, et al. Hypomagnesemia inhibits nitric oxide release from coronary endothelium: Protective role of magnesium infusion after cardiac operations. Apr 1998. Ann Thoracic Surg. https://www.annalsthoracicsurgery.org/article/S0003-4975(98)00020-4/fulltext
Read the Myocarditis and COVID series here > Myocarditis series








Comments
Post a Comment