Post COVID management protocol: What you need to know (September 2022)
Background
COVID–19 disease caused by SARS-CoV-2 Coronavirus is relatively a new disease, with fresh information being known on a dynamic basis about the natural history of the disease, especially in terms of post-recovery events.
After acute COVID-19 illness, recovered patients may continue to report wide variety of signs and symptoms including fatigue, body ache, cough, sore throat, difficulty in breathing, etc.
Scope
This document provides an integrated holistic approach for managing patients who have recovered enough from COVID. The recovery period is likely to be longer for patients who suffered from more severe form of the disease and those with pre-existing illness.
Post-COVID Protocol

If you have symptoms that include major shortness of breath, cough with blood in it or pain on one side when you take a deep breath, it could be due to a late pulmonary embolism or a blood clot going to the lungs. Please visit your medical doctor or the nearest 24-hr medical emergency center immediately.
COVID–19 disease caused by SARS-CoV-2 Coronavirus is relatively a new disease, with fresh information being known on a dynamic basis about the natural history of the disease, especially in terms of post-recovery events.
After acute COVID-19 illness, recovered patients may continue to report wide variety of signs and symptoms including fatigue, body ache, cough, sore throat, difficulty in breathing, etc.
Scope
This document provides an integrated holistic approach for managing patients who have recovered enough from COVID. The recovery period is likely to be longer for patients who suffered from more severe form of the disease and those with pre-existing illness.
Post-COVID Protocol
The FLCCC (Front Line COVID-19 Critical Care Alliance) was formed by leading critical care specialists in March 2020, at the beginning of the Coronavirus pandemic, dedicated to developing highly effective treatment protocols to prevent the transmission of COVID-19 and to improve the outcomes for patients ill with the disease.
Though there are many long haul COVID treatment protocols out there, we consider and recommend the I-Recover for Long Haul as one of the best.
Given the lack of clinical trials of long-haul COVID-19 syndrome, these recommendations are based on the abnormal changes within the body associated with the COVID-19 disease and post viral illnesses along with the collective experience of FLCCC members.
This protocol has also been used to treat post-vaccine inflammatory syndromes with similar success. As with all FLCCC Alliance protocols, the components, doses, and durations will evolve as more clinical data accumulates.
The I-Recover protocol for long haulers has been updated and below is their latest version (version 3: Sep 6, 2022). Do not confuse this I-Recover protocol for long haul COVID with another I-Recover protocol for post-vaccine syndrome that was launched in May 2022, by FLCCC. One is for post covid long haulers and the other, for post vaccine syndrome.
Treatment must be individualized according to each patient’s presenting symptoms and disease syndromes. It is likely that not all patients will respond equally to the same intervention; a particular intervention may be life-saving for one patient and totally ineffective for another. Early treatment is essential; it is likely that the response to treatment will be attenuated when treatment is delayed.

First-line treatments (In order of priority; not all required):
- Prednisone: 10–15mg daily for 3 weeks. Taper to 10mg for three days, then 5mg for three days and then stop.
- Ivermectin: 0.2 - 0.3 mg/kg body weight. (Find a Doctor)
- Low dose naltrexone (LDN): Begin with 1 mg daily and increase to 4.5mg as required. May take 2–3 months for full effect.
- Intermittent daily fasting and/or periodic daily fasts: Fasting promotes autophagy, the body’s protective mechanism to remove misfolded, foreign and damaged proteins. It also promotes mitophagy and the release of stem cells. It is likely that promoting autophagy will aid in the removal of the spike protein. NOTE: Hydroxychloroquine inhibits autophagy and should be avoided in patients undergoing intermittent fasting.
- Spermidine and/or Resveratrol: These compounds have been demonstrated to augment autophagy. Wheatgerm, mushrooms, grapefruit, apples and mango are high natural sources of spermidine. A bio-enhanced formulation containing trans-resveratrol from Japanese Knotwood Root appears to have good bio-availability.
- Melatonin: 8mg at night (slow release/extended release preferred) with attention to sleep hygiene. Increase dose from 1mg as tolerated (may cause severe nightmares at high dosages).
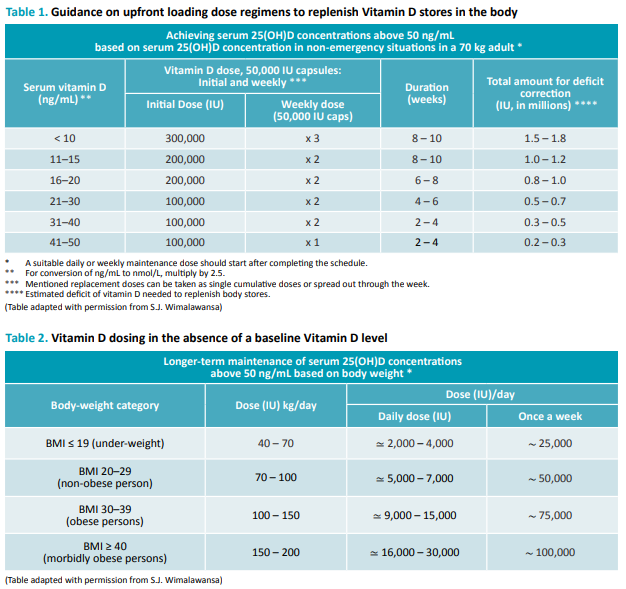
- Vitamin D: The majority of those with post-COVID-19 syndrome continue to have hypovitaminosis D. See tables 1 or 2 for vitamin D supplementation.
- Omega-3 fatty acids: Vascepa, Lovaza or DHA/EPA 4g per day. Omega-3 fatty acids play an important role in the resolution of inflammation by inducing resolvin production. [Ref, Ref]
- Curcumin (turmeric): 500 mg twice daily. Has anti-inflammatory and immunomodulating properties and has been demonstrated to repolarize macrophages.
- Aspirin — 81 milligrams a day.
2nd Line Therapies
If symptoms do not improve after 1-2 weeks continue steroids, Omega-3 fatty acids and LDN and add second line therapies as below.
- Fluvoxamine (low dose): 25mg once daily. Stop if the symptoms increase. Caution with the use of other antidepressants and psychiatric drugs. Taper and discontinue once symptoms improve.
- Hydroxychloroquine (HCQ): 200 mg twice daily for 1-2 weeks, then reduce as tolerated to 200 mg daily. HCQ is the preferred second line agent. With long term usage, the dose should be reduced (100 mg or 150 mg daily) in patients weighing less than 61 kg (135 lbs).
- Intravenous Vitamin C: 25 g/week, together with oral Vitamin C 1000 mg (1 gram) 2-3 times daily. Oral Vitamin C is important to provide nutrients for the microbiome. Total daily doses of 8-12 g have been well-tolerated, however chronic high doses have been associated with the development of kidney stones, so the duration of therapy should be limited. Wean IV Vitamin C as tolerated.
- Mitochondrial energy optimizer with pyrroloquinoline quinone (e.g., Life Extension Energy Optimizer or ATP 360®).
- N-acetyl cysteine (NAC): 600-1500 mg/day.
3rd Line Therapies
- Maraviroc (Pfizer’s CCR5 antagonist): 300mg PO twice a day If 6–8 weeks have elapsed and significant symptoms persist, consider either getting an InCellDx test to assess long hauler index profile prior to initiating or can consider initiating empirically. Note maraviroc can be expensive and it has risk for significant side effects and drug interactions.
- Non-invasive brain stimulation (NIBS): using transcranial direct current stimulation or transcranial magnetic stimulation. NIBS is painless, extremely safe, and easy to administer. NIBS is offered by many Physical Medicine and Rehabilitation Centers. Patients may also purchase an FDA-approved device for home use.
Optional adjunctive therapies (in order of priority)
- Nigella Sativa: which like curcumin has anti-inflammatory and immunomodulating properties.
- Atorvastatin: 20–40mg once daily. Caution in patients with Postural Orthostatic Tachycardia Syndrome (POTS); may exacerbate symptoms.
- Kefir, probiotic yogurt and/or Bifidobacterium Probiotics (e.g., Daily Body Restore) together with Prebiotics (e.g. XOS Prebiotic, Bio Nutrition Pre-Biotic) to normalize the microbiome. Prolonged dysbiosis has been reported following COVID-19 infection.
- Behavioral modification, mindfulness therapy and psychological support may help improve survivors’ overall well-being and mental health.
- Luteolin 100–200mg day or Quercetin 250mg day (or mixed flavonoids). Luteolin and quercetin have broad spectrum anti-inflammatory properties. These natural flavonoids inhibit mast cells, and have been demonstrated to reduce neuroinflammation. [R]
- H1 receptor blockers (for mast cell activation syndrome): Loratadine 10mg daily, or Cetirizine 5–10mg daily, or Fexofenadine 180mg — daily.
- H2 receptor blockers (for mast cell activation syndrome): Famotidine 20–40mg, or Nizatidine 150mg — twice daily as tolerated.
- Montelukast: 10mg/day (for mast cell activation syndrome). Caution as may cause depression in some patients.
- Anti-androgen therapy: Spironolactone 50–100mg twice a day, and Dutasteride 1mg daily.
Mast cell stabilisers: rupadatadine, quercetin or luteolin.
Moving Forward
One of the pandemic’s few bright spots is the way it’s accelerated telehealth services. Patients now can have unprecedented access to a broad range of healthcare providers across the nation.
Find healthcare providers:
- List of Doctors that will prescribe Ivermectin and Hydroxychloroquine
- List of Pharmacies that will fill Ivermectin
- www.ifm.org/find-a-practitioner (Functional Medicine)
- Post-COVID Care Centers (PCCC) by Survivor Corps








Comments
Post a Comment