MATH+ Protocol for COVID-19 and Dr Paul Marik
The MATH+ Protocol Story
January, 2020. Dr. Paul E. Marik, Professor of Medicine and Chief of the Division of Pulmonary and Critical Care Medicine at the Eastern Virginia Medical School in Norfolk, Virginia, creates a COVID-19 hospital treatment protocol for the medical school. Called the EVMS protocol, it is based on Dr. Marik’s safe, effective treatment protocol for sepsis — the famous “Marik Cocktail” of intravenous Hydrocortisone, Ascorbic Acid, and Thiamine (HAT).- CITRIS-ALI, a large double-blind placebo controlled trial of high dose ascorbic acid (AA) in Acute Respiratory Distress Syndrome (ARDS) found that mortality decreased and ICU length-of-stay were markedly reduced in the treatment group.
- The reasons for the lack of immediate adoption of this therapy in ARDS can only be explained by the fact that the original primary outcome analysis failed to account for all the early excess deaths in the control group, where no Sequential Organ Failure Assessment (SOFA) score was assigned to the patients who died. A subsequent letter to the editor demanded an analysis accounting for the early deaths. The study authors complied, and reported the primary outcome of SOFA score to be statistically significantly decreased at 96 hours. Thus CITRIS-ALI, although inexplicably initially portrayed as a negative trial, was later found to be profoundly positive in terms of achieving its primary outcome and important secondary outcomes.
Update: Vitamin C and Sepsis: Surprising results from the LOVIT trial (June 2022, NEJM)
March 13, 2020. The United States declares a national emergency in response to the pandemic. New York City becomes the first major “hot spot” in the country, where 20% of hospitalized cases develop acute respiratory failure (ARF) requiring ICU admission. Based on the assumption that COVID-19 represents a viral pneumonia and no anti-coronaviral therapy exists, nearly all national and international health care societies advocate a primary focus on supportive care, avoiding therapies outside of randomized controlled trials, with specific recommendations to avoid the use of corticosteroids. This recommendation stands in opposition to the EVMS protocol which includes hydrocortisone. Inexplicably high mortality rates are reported, with frequent prolonged durations of mechanical ventilation (MV), even from centers expert in supportive care strategies.
March 16–21, 2020. New York City internist Keith Berkowitz searches for a way to treat his patients who contract COVID. He finds the EVMS protocol and calls Dr. Marik, who suggests he also talk to Dr. Kory. Convinced of the benefits of intravenous AA, Dr. Berkowitz wants to get word of the new treatment protocol to government officials and the media. He calls his longtime patient, former CBS News Correspondent Betsy Ashton, for advice. Newly locked down in New York City, Betsy is eager to help him reach out to major media in an effort to potentially save thousands of lives. Dr. Berkowitz urges Drs. Marik and Kory to recruit more critical-care experts to the cause.
March 22–28, 2020. Dr. Howard Kornfeld, a board-certified emergency medicine specialist best known for his Recovery Without Walls pain control clinic in Mill Valley, California, also independently researches and finds the EVMS protocol. He contacts Dr. Marik. Dr. Kornfeld is certain that the protocol, with its enormous potential for saving lives, needs to reach governors and the media. He contacts writer Joyce Kamen, who heads the Kamen Creative Public Relations firm in Cincinnati, Ohio. Kamen’s husband, Dr. Fred Wagshul, is a Pulmonologist and Medical Director of the Lung Center of America, and is also a clinical instructor at the Wright State University School of Medicine in Dayton, Ohio. Both Joyce Kamen and Dr. Wagshul join to help spread the word of the highly promising protocol. Dr. Marik invites Dr. G. Umberto Meduri, Professor of Medicine, Div. of Pulmonary, Critical Care and Sleep Medicine, at the University of Tennessee Health Science Center in Memphis, Tennessee; Dr. Joseph Varon, Chief of Staff & Chief of Critical Care at United Memorial Medical Center in Houston, Texas; and Dr. José Iglesias, Associate Professor of Medicine, Hackensack Meridien School of Medicine at Seton Hall, Department of Nephrology & Critical Care, Community Medical Center, Department of Nephrology, Jersey Shore University Medical Center, Neptune, New Jersey, to join the group. All three, like himself, are leading ascorbic acid experts and are eager to help Dr. Marik create an effective treatment for the challenging new disease that threatens millions around the globe.
March 31, 2020. Betsy Ashton writes the first press release about the new treatment entitled “Hospitals use IV’s of Vitamin C and other low-cost, readily available drugs to cut the death rate for COVID-19 and the need for ventilators.” She reports that Dr. Paul Marik has treated four seriously ill COVID patients, including an 86-year old man suffering heart disease, who was admitted to the hospital on 100% oxygen — a patient not likely to survive. All four survived. Dr. Joe Varon’s sixteen COVID patients had gotten off ventilators in 24 hours instead of 10–21 days. Joyce Kamen pens and publishes a similar article on medium.com the next day.
April 6, 2020. Betsy Ashton writes, and Joyce Kamen designs, the first press releases of the newly formed FLCCC group. The releases urge immediate adoption of the early intervention protocol to reduce the need for ventilators and prevent mortality from COVID-19 disease. They report that Dr. Paul Marik has treated seven seriously ill COVID patients in his Norfolk, Virginia, hospital, and Dr. Joe Varon has treated twenty-four at United Memorial Medical Center in Houston, Texas. Both doctors used the new formula and all patients survived. Joyce Kamen then sets up Facebook and Twitter accounts for the group and posts the releases online. Dr. Keith Berkowitz, through one of a large circle of high-profile contacts, sends the protocol to the White House COVID-19 response team headed at the time by Jared Kushner. This would be the first of four instances where high profile members of the medical, political, and media community would send the protocol to the White House for consideration.
MATH+ Protocol
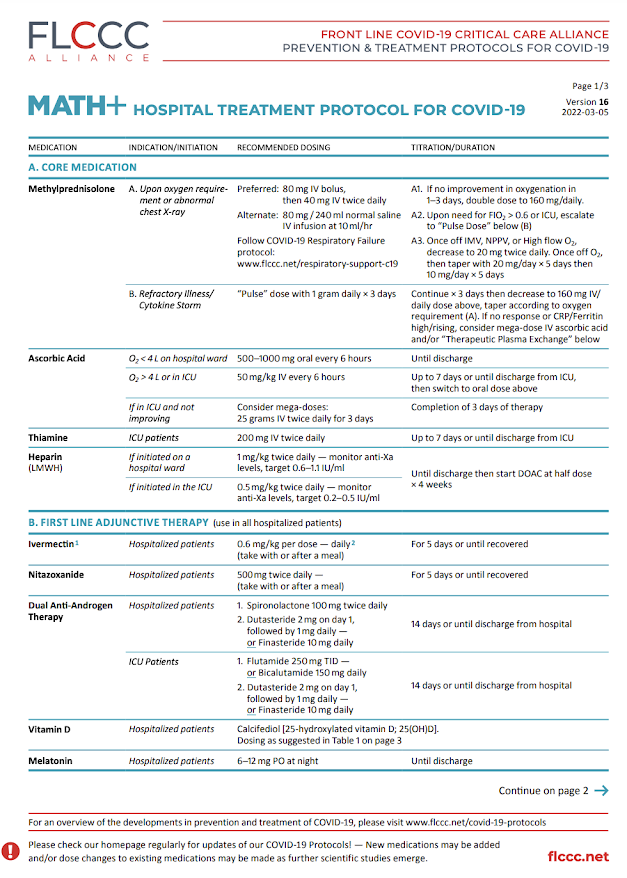
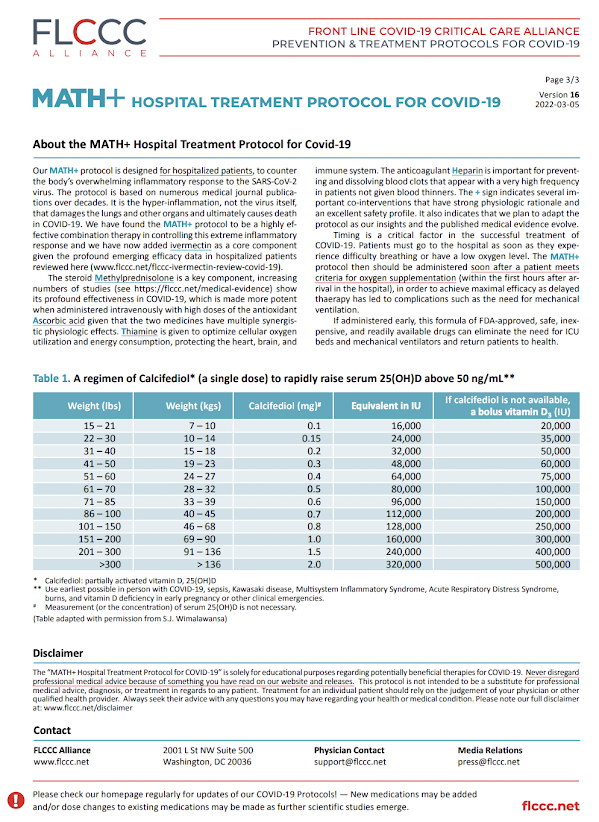
The MATH+ Hospital Treatment Protocol for COVID-19 is designed for hospitalized patients, to be initiated as soon as possible after they develop respiratory difficulty and require oxygen supplementation. The three core pathophysiologic processes that have been identified are severe hypoxemia, hyperinflammation, and hypercoagulability. This combination medication protocol is designed to counteract these processes either through the use of single agents or in synergistic actions. A unique insight into this disease made by members of our group is that the majority of patients initially present with an inflammatory reaction in the lungs called “organizing pneumonia,” which is the body’s reaction to injury and is profoundly responsive to corticosteroid therapy. If the organizing pneumonia response is left untreated or presents as a rapidly progressive sub-type, a condition called Acute Respiratory Distress Syndrome (ARDS) follows.The two main therapies that can reverse and/or mitigate the extreme inflammation causing ARDS are the combination of the corticosteroid Methylprednisolone and the antioxidant Ascorbic acid, which is given intravenously and in high doses. Both of these medicines have multiple synergistic physiologic effects and have been shown in multiple randomized controlled trials to improve survival in ARDS, particularly when given early in the disease. Thiamine is given to optimize cellular oxygen utilization and energy consumption, protecting the heart, brain, and immune system. Given the numerous clinical and scientific investigations that have demonstrated consistent, reproducible, and excessive levels of hyper-coagulation, particularly in the severely ill, the anticoagulant Heparin is used to both prevent and help in dissolving blood clots that appear with a very high frequency. The “+” sign indicates several important co-interventions that have a combination of strong physiologic rationale with existing or emerging pre-clinical and clinical data to support their use in similar conditions or in COVID-19 itself, and all with a well-established safety profile. Such adjunctive therapies are continuously being evaluated and amended as the published medical evidence evolves.
Timing is a critical factor in the efficacy of MATH+ and to achieving successful outcomes in patients ill with COVID-19. Patients must go to the hospital as soon as they experience difficulty breathing or have a low oxygen level. The MATH+ protocol should be administered soon after a patient meets criteria for oxygen supplementation (within the first hours after arrival in the hospital), in order to achieve maximal efficacy. Delayed therapy can lead to complications such as the need for mechanical ventilation. If administered early, the MATH+ formula of FDA-approved, safe, inexpensive, and readily available drugs may eliminate the need for ICU beds and mechanical ventilators and return patients to health.
Current MATH+ protocol: version 16, updated on Mar 5, 2022
A. CORE MEDICATION
Methylprednisolone
A. Upon oxygen requirement or abnormal
chest X-ray
- Preferred: 80mg IV bolus, then 40mg IV twice daily
- Alternate: 80mg / 240ml normal saline IV infusion at 10ml/hr
- Follow COVID-19 Respiratory Failure protocol: www.flccc.net/respiratory-support-c19
A1. If no improvement in oxygenation in
1–3 days, double dose to 160mg/daily.
A2. Upon need for FIO2 > 0.6 or ICU, escalate
to “Pulse Dose” below (B)
A3. Once off IMV, NPPV, or High flow O2,
decrease to 20mg twice daily. Once off O2,
then taper with 20mg/day × 5 days then
10mg/day × 5 days
B. Refractory Illness/
Cytokine Storm
- “Pulse” dose with 1 gram daily × 3 days
- Continue × 3 days then decrease to 160mg IV/ daily dose above, taper according to oxygen requirement (A). If no response or CRP/Ferritin high/rising, consider mega-dose IV ascorbic acid and/or “Therapeutic Plasma Exchange” below
Ascorbic Acid
O2 < 4L on hospital ward
- 500–1000mg oral every 6 hours
- Until discharge
- 50mg/kg IV every 6 hours
- Up to 7 days or until discharge from ICU, then switch to oral dose above
If in ICU and not
improving
- Consider mega-doses: 25 grams IV twice daily for 3 days
- Completion of 3 days of therapy
Thiamine
ICU patients
- 200mg IV twice daily
- Up to 7 days or until discharge from ICU
Heparin
(Low Molecular Weight Heparin)
If initiated on a
hospital ward
- 1mg/kg twice daily — monitor anti-Xa levels, target 0.6–1.1 IU/ml
- Until discharge then start DOAC at half dose × 4 weeks
If initiated in the ICU
- 0.5mg/kg twice daily — monitor anti-Xa levels, target 0.2–0.5 IU/ml
- Until discharge then start DOAC at half dose × 4 weeks
B. First Line Adjunctive Therapy (use in all hospitalized patients)
Ivermectin
- Hospitalized patients
- 0.6 mg/kg per dose — daily 2 (take with or after a meal)
- For 5 days or until recovered
Nitazoxanide
- Hospitalized patients
- 500mg twice daily — (take with or after a meal)
- For 5 days or until recovered
Dual Anti-Androgen
Therapy
- Hospitalized patients
- 1. Spironolactone 100mg twice daily
- 2. Dutasteride 2mg on day 1, followed by 1mg daily — or Finasteride 10mg daily
- 14 days or until discharge from hospital
- ICU Patients
- 1. Flutamide 250mg TID — or Bicalutamide 150mg daily
- 2. Dutasteride 2mg on day 1, followed by 1mg daily — or Finasteride 10mg daily
- 14 days or until discharge from hospital
Vitamin D
- Hospitalized patients
- Calcitriol: 0.5mcg on day 1, then 0.25mcg daily
- 7 days
Melatonin
- Hospitalized patients
- 6–12mg PO at night
- Until discharge
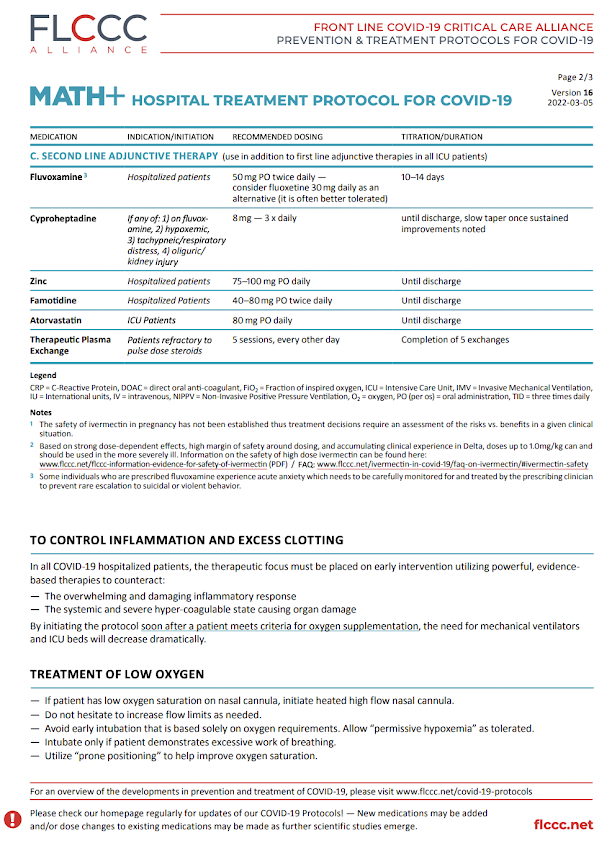
C. Second Line Adjunctive Therapy (use in addition to first line adjunctive therapies in all ICU patients)
Fluvoxamine
- Hospitalized patients
- 50mg PO twice daily — consider fluoxetine 30mg daily as an alternative (it is often better tolerated)
- 10–14 days
Cyproheptadine
- If any of: 1) on fluvoxamine, 2) hypoxemic, 3) tachypneic/respiratory distress, 4) oliguric/ kidney injury
- 8mg — 3 x daily
- until discharge, slow taper once sustained improvements noted
Zinc
- Hospitalized patients
- 75–100mg PO daily
- Until discharge
Famotidine
- Hospitalized Patients
- 40–80mg PO twice daily
- Until discharge
Atorvastatin
- ICU Patients
- 80mg PO daily
- Until discharge
Therapeutic Plasma
Exchange
- Patients refractory to pulse dose steroids
- 5 sessions, every other day
- Completion of 5 exchanges
For post-covid or long covid syndrome, check out Post-COVID Treatment Protocol.







.png)
Comments
Post a Comment